Going into the 2022 Hardrock 100 I had grand aspirations and goals (which included a sub-30h finish). The quick answer is things went about as well as it could have, but not as well a I dreamed it would. I’ve always set big goals for myself, many of them born out of insufficiency and insecurities from past lives; You’re too slow, you’re not strong enough, you’re too short, too awkward, not smart enough… Every person who steps foot on the line at Hardrock has dealt with their own challenges to get there and most likely still carries some of those challenges through the race and life in general. To claim we are all equal is a lie, we all are unique and none of us will ever have the same experience and that’s perfectly ok. Something I’ve struggled with for a long time is the idea that if I worked hard enough I could achieve some of the lofty aspirations, maybe not Killian level, but pretty high. 16 years after I started ultrarunning, I’m finally accepting that’s just not the case. To be clear, I’m not looking for a pity party, but rather through a recognition of my own weaknesses (and also my strengths), I can become the best version of that self and achieve whatever my personal limits may be.
Pre-race nervous shakeout and relaxation up at Hematite Lake with Jason.
Ok, back to Hardrock. Last year (2021) I went into the race determined to push hard and really find my potential, and a new level of success (time and place). What ended up happening was out running my capabilities early and suffering through the last 1/3 of the experience. 2022 brought a much different approach, listen to my body, be grateful for every experience (good and bad) and to enjoy a much as possible. In the past what’s done me in is running to others expectations, trying to keep up with others (not myself) and not fully listening to my body. The biggest challenge was admitting that my airways and lungs are my weak point and will always limit what I can do, especially at high altitude. This is not new (Nolans, past Hardrocks, 24h 14ers, Elks and others), but it’s been a hard thing to admit that it’s not something I can train past or “overcome”. I’ve found ways to cope and build other strengths; getting faster downhill, increasing overall fitness, running longer and slower, but none of these will ever remove this weak link of mine.
Cresting the Putnam Divide early in the race, mm10.The infamous Island Lake near Grant Swamp Pass, always a worthwhile visit.
I slept terribly the week before the race (another temporary challenge) and work stresses had me a bit out of sorts, not the best way to start a super hard 100mi race. But I was promised to spend a long weekend running around some is the most beautiful mountains, with a crew of great friends, I was lucky indeed. The first climb went by smoothly, as I focused on just taking in as much of the experience as possible, soon finding myself in the familiar position of leap-frogging with Darcy. Maggie soon caught up to us not too much later and the three of us would spend the next 30miles leap frogging back and forth (them on the ups, me on the downs). Every time I rolled through an Aid Station the friendly faces would provide a boost, finally getting to see my crew in Telluride (mm28). The stoke was high, I was still feeling great and just doing my own thing. As we (Darcy, Maggie and I) left Telluride a big storm dropped in and pummeled us with rain and hail for 45min, but it was fine, we were below treeline and safe, just moist. The ominous skies still threatened as we approached Kroger’s Canteen. A couple of perogies, some coke and off down to Ouray I went. I was finding my own rhythm, playing to my strengths, listening to my body and just letting the miles roll by. Ouray was a wild circus full of energy. Tons of friends, spectators and confused tourist everywhere. For the first time at Hardrock I left an Aid Station without a pacer, focusing just on myself and the mountain experience I was seeking. Darkness fell as I led a group of us up and over Engineer Pass and down into Animas Forks. The aid station was a bit of a mess and I almost ran right by my crew without either of us realizing it. After a quick change into my nighttime gear, Jason and I were off to Handies, my white whale.
Nearing the summit of Virginius Pass, just after one thunderstorm had passed over, right before another one was about to hit.Crew stop and refeul in Ouray before heading up to Engineer Pass.
As we headed up the Grouse saddle the work stress and lack of sleep were catching up with me and I’d spend the next 5h a walking zombie. My lungs strained in the cold air and I knew if I didn’t slow I was at risk of damaging the rest of my race, so upwards we crawled. After much bitching and moaning on my part (Jason was great) we made it to Burroughs AS where Jesus greeted us with open arms (no I want hallucinating yet). I kept trudging forward at what felt like a slow crawl, picked up Gwen at Sherman, then slowly staggered my sleepy way to sunrise at the pole creek divide. As the sun illuminated the surrounding mountains, my spirits began to lift. Gwen commented that she knew I was back when I made some very juvenile comment that only a 12yo would make, oops. So we ran (some) and walked (a bunch), enjoying what was a mostly lovely day. I probably groaned a bit when we hit the precipitous descent into Cunningham, but that meant only 1 AS left! I did my best to keep things fun at our last crew exchange, but I was just a wee bit tired, so who knows how well that came off. Bailee and I set off at a slow trudge up Dives/Little Giant, trying to keep my breathing in check (and not set off my asthma), but also wanting to get done. As we crested the top, I took one last look back at Green Mt and finally let myself believe I was going to get it done.
Full moon rising as Jason and I make our way over Handies Peak at 14000ft.Down into Maggie we go, endless wildflowers all around and Day 2 sunshine.
Still kinda smiling and kinda having fun, final climb up and over Dives/Little Giant, almost done!
Whatever pain and fatigue I felt didn’t matter, all I had to do was will my way downhill to the finish. We ran as fast as I could down the technical descent, taking a few walk breaks to catch my breath. We stomped through the river and hit the final few miles into town, running into Jefferson along the way. I ran as hard as my lungs would allow, but with two miles to go I was sent into a coughing fit, diaphragm spasms and promptly threw up. This was the first time that’s ever happened during a race. Once I stopped coughing I felt fine, so we jogged it in. As we cruised through town we were greeted by many familiar faces, including my crew. It felt really good to kiss the rock for the 3rd time, but it felt even better to be in good spirits (despite puking) and to have enjoyed the experience (for the most part).
Finish line vibes.
The rest of the day was spent on a quick nap, cheering on the multitude of friends finishing that afternoon/evening and eating all the food I could find (burrito, 2x burgers, cookies, soup, etc). My training had succeeded, my legs held up (my legs are never my limiting factor at elevation), and other than my 5h sleepy stretch so had my energy levels. I’ve learned that no matter how hard I train, at Hardrock I can’t outrun my lungs, so sub-30h may never be in the cards for me, and I’m ok with that. I had a great run with my good friends, and that is really what I wanted most out of the experience. Sure it would be awesome to run faster, but after 34:38, 33:52 and 33:10 finishes I’ve accepted this is who I am. On to other new adventures, different races and to enjoy crewing my friends at Hardrock in future years, where I get to eat all the food, take a few naps and not run 100miles of that crazy course all at once. Big thanks to Vfuel for supporting my training and my Hardrock adventure, all the Rocky Mountain Runners for the training miles shared and my friends and crew for dragging my sometimes grumpy ass around the San Juans yet again.
The question I’ve received many times is what does Omicron mean for the end of the pandemic and the future of the vaccinated? The short answer is, anyone who tells you they know what is going to happen, when things will end or what the future holds is lying. While there are definitely signs of what the future of Omicron and the pandemic (maybe turning endemic) hold, Nature does not listen to our whims and there are biologically and epidemiologically still several paths we could travel down. The following blog is a departure from many of my previous writings in that it’s mostly my opinions and thoughts on these topics, lots of hypothesis, many of which are far from proven, but are still none the less backed up by scientific evidence and general biological principles. Welcome to the inner wanderings of my mind…..
Omicron Spread and Vaccines: I’ll start by diving into why is Omicron spreading so fast, how might it be different and what does it mean for the future of the vaccine programs. The Omicron variant was first detected in South Africa in November 2021 (though the variant could have originate elsewhere), and what made it so unusual and worrisome was it contained 53 (!) mutations from the original founder strain, an extremely high number for a coronavirus. Hypothesis are currently that this virus must have evolved on it’s own in a long term reservoir (either immunocompromised host or animal) separate from Beta or Delta because it doesn’t closely resemble those two variants, but these are just hypothesis at the moment. What makes Omicron so successful is that these mutations appear to allow it to more efficiently bind to and enter human cells of the upper airway. This combined with the evidence that several of the mutations also interfere with the binding of some antibodies created by the vaccines (and previous infections), mean that our barrier to preventing initial infection with Omicron are torn down a bit more, but our protection is not lost! So while vaccine detractors will point to vaccinated people becoming infected (which is true), there is a lot of real world evidence coming out that if you received a Covid vaccine (booster even better) you’re MUCH less likely to suffer severe disease or be hospitalized, which after all is what worries us the most. Part of the reason for this is that even though your immune defenses can’t prevent the initial infection, there appears to be enough cross-reactivity between existing immunity and Omicron that the body gets a jump start on fighting the infection, and as such has a much easier time controlling the disease. I attribute my current case of Omicron being mild to these advantages (in addition to being young-ish and healthy). We also have the good fortune that Omicron appears to not cause as severe disease (on average) when compared to Delta. A current working hypothesis is that what makes Omicron more infectious, may also mean it doesn’t damage the pulmonary tissue as much. After all, a virus’s main goal is to replicate and spread, and a dead host is not useful for spreading a virus. Successful viruses infect a host efficiently, replicate quickly and allow that host to spread the virus to other hosts. This is exactly what Omicron appears to be doing, and what also brings us to the next topic, Endemicity.
Endemicity? The hope has always been we get to a place through vaccination, medications and natural immunity where we can live in more of a steady state with SARS-CoV-2. What this would include is the virus being a normal part of life, circulating within the population, not causing massive outbreaks, overflowing hospitals, killing hundreds of thousands and infecting millions each month. Obviously we’re not there yet as we still see massive numbers of new infections each day, a lot of hospitalizations and far too many dying (as of 1/24, >1000/day US). But what people are starting to allow themselves to talk about with Omicron is the potential that with how fast Omicron is spreading and the more widespread availability of vaccines, that maybe moving from the current pandemic to SARS-CoV-2 being endemic is possible.
For this to happen, enough people would have to be immune and/or refractory to severe infection that the virus is no longer a concern for most people (or our hospital system). The current variant, being less severe (on average) and far less severe (on average) in vaccinated individuals does look like it could push us in that direction. The trouble with proclaiming the end of the pandemic pre-maturely is that no one can tell you for certain that as the virus infects hundreds of millions more people in it’s push to endemicity, it won’t mutate again to become more severe/deadly. While the idea that there aren’t direct biological evolutionary pressures pushing the virus to be more effective at killing the host…mutations can be random and don’t always follow that path. But if Omicron continues on it’s current path (BIG IF) and infects much of the population in the coming months then maybe the number of new infections in each outbreak will greatly dwindle, our hospitals won’t overflow with severely ill patients and maybe we can move forward with thinking of SARS-CoV-2 as just another cold virus…..just maybe. Our work is still not done, hundreds of millions will still get infected in the coming months/year and many will die sadly. Our job right now is to arm ourselves with as many tools to fight the virus as possible (vaccinate the world, stay healthy, wear a mask to reduce exposure, keep researching new medications) and to protect those who are still at the highest risk of severe infection.
Eric is an Immunologist and Infectious Diseases Scientist based in Boulder, CO. The thoughts in this blog are his own and are by no means proclamations of certainty, but rather musings and hypothesizing.
Sciencing the shit outta stuff, that’s how we do it.
Hello my name is Eric Lee and I’m an Asian American (technically multi-racial). Recent event have really pushed to the forefront of thought my personal relationship with racial bias, racism and the systemic social issues that plague our country. As an Asian American I’ve been exposed to my share of negative racial commentary throughout life; comments about eyes, color, language, driving ability, eating habits, how we name our children, penis size (yes I’m being serious), disparaging looks and on and on. Though at the same time I must also admit the privilege I’ve had growing up in a middle class community. Most of these taunts and racial slurs have come from stupid and non-physically threatening sources. Meaning, I never had to fear for my life or feared someone was going to do me physical harm as part of this. Having grown up in an immediate community where violence was not the norm, where law enforcement was not prone to profile individual POC, I was privileged that the abuse was only verbal and emotional, not physical. This may not sound like much of a privilege, but I think we are all realizing (because of recent and ongoing events), that this simple factor IS a privilege.
Which brings me to the much messier question, how have I been a part of them problem for all these years. While Asian Americans have by no means had an easy history in the US, we’ve greatly benefited from the civil rights movements while not being as visible on the front lines. Also, because of the backing of strong Asian economies many have been fortunate to position themselves in more affluent settings. While this doesn’t change the profiling or underlying racial issues, it does ease the reactions/interactions that we’ve endured. I will never know what it’s like to be an African American living in a lower socioeconomic neighborhood, who fears being arrested/beaten or worse every time they leave their home to go to the store, work or school. I will never truly know the frustration of fighting for equal rights for decades, to seemingly make little headway. One of my first exposures to the unrest associated with racial injustice was watching Los Angeles burn in 1992 during the Rodney King riots (and hearing the rise of gangsta rap). As a 10yo I didn’t fully grasp the situation, but the image is still deeply imprinted in my mind. Do I like that these protests have turned violent (whether it’s the protesters or other agitators not related, remains to be seen)? No, but it doesn’t surprise me one bit. If I’d been trying to calmly, logically and peacefully protest and make my voice heard only to be brushed aside time and again, I too would have little faith in a system that keeps promising things will change but never delivering that change. Whether you like it or not, you can’t help notice what’s going on, and the protesters and voices screaming for change have your attention. I know they’ve got mine, and while I consider myself an educated and empathetic human, they’ve got me reconsidering my place in perpetuating the racial inequality that continues to persist. We can all be better, we can all do better, and we must.
By now some
of you know that this past weekend I took a very short trip back to see family
in California, traveling by plane both directions. I know many people are itching
to hop back on a plane, travel and to get away from it all. So to help everyone
make a more informed choice I’ll lay out what I did to mitigate much of the
risk of flying and how my experience went navigating all the public spaces that
come with traveling to a different state. If you want to ask (or scold if you
must) me about my personal reasons for doing this you are more than welcome to
send me a DM or email and I’ll respond individually with that information, but
its personal and thus not suited for a public forum and not the point of this
writeup.
Every departing flight from Denver between 6p-11p on a Friday afternoon….. wow!
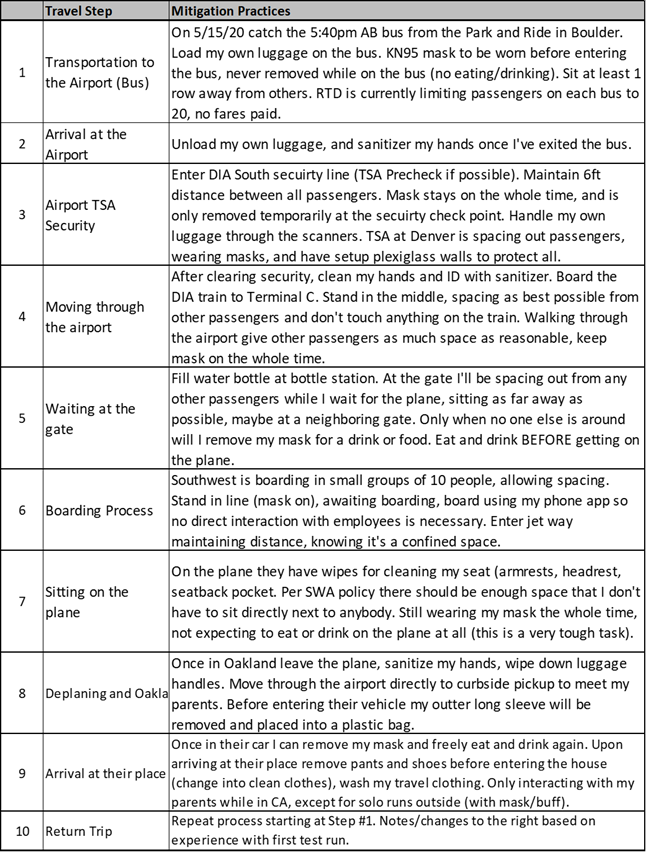
My Mitigation Plan For me this whole process was a test of my ability to creation infectious disease mitigation plans, a skill I learned and honed working in tuberculosis and HIV labs for many years. So I did not simply hop on a plane and wait to see what happened, I had a whole step by step plan of all the risks involved with travel, how I would protect myself and how I would act in certain situations. Below is my initial plan that I laid out BEFORE traveling, and it is VERY conservative.
Now on to the reality of the situation and what I observed and found. I’ll lump both my flights together as a way to give the sum of a couple different experiences for each step listed above.
The whole journey for me started in Boulder boarding the RTD AB bus which heads to the airport. Under normal circumstances these buses are packed and can be standing room only, but right now RTD is limiting the number of passengers on each bus to <20, has suspended fare collections and is requiring all drivers/passengers to wear face coverings. When I got on it was apparent it was going to be a quiet trip, just myself and one other person headed to the airport!
On my way to the airport on RTD, the bus is empty except for one other person and the driver.
The
Airport
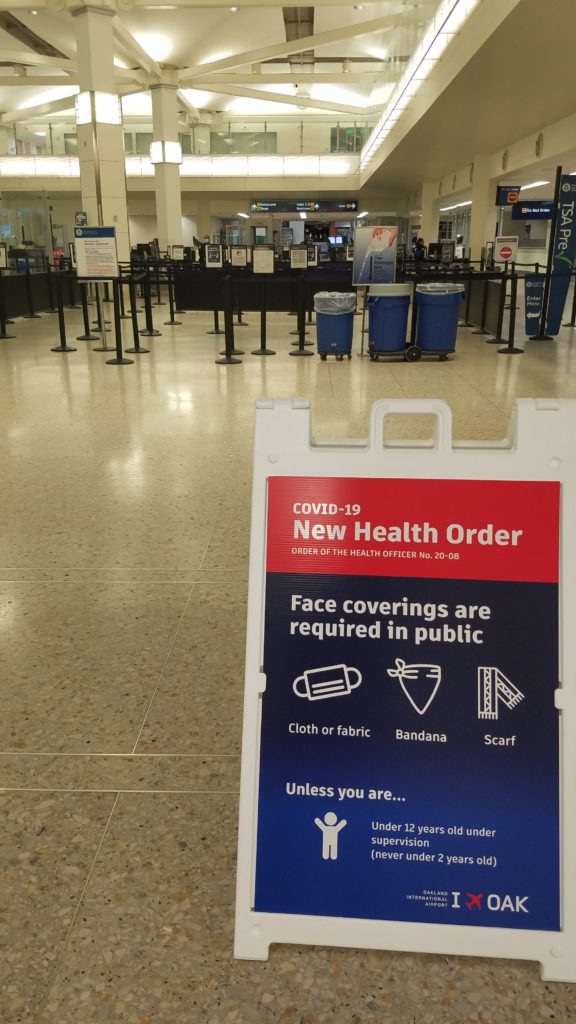
Needless to say the ride went smoothly, but I still kept my mask on the whole time. Arriving at the airport I unloaded my own bag and headed up the escalators to security. I was astonished to find 1 person (TOTAL) in line in front of me. I walked up to TSA precheck, handed the security office my ID, she didn’t even request I remove my mask (though they did in Oakland), then I passed on through. In Oakland they didn’t even have a precheck lane running, instead they specially escorted me through normal security (shoes on, liquids in the bag). After security I sanitized my hands and ID and headed to the gate. I only passed by a few people, almost all of whom were wearing masks of some variety (they are mandatory in the airport). As I approached the gate I was astonished to see the bar at Timberline Steaks (Denver) was open and seating patrons at the bar/restaurant? I filled my water bottle, washed my hands and headed over to the gate. At the gate there were only about 20 people heading to Oakland, and 30 people on the return flight, for planes that have a capacity for 140 people. I found a spot at the gate spread out between others, which was easy, and sat down to eat my snacks and grab some water before the flight. This was the first time I removed my mask and it was only for a few minutes in a safely spaced out area. While waiting for my first flight an SWA worker came and sat right behind me, no attempts to space out, and while waiting for my second flight a woman came and stood right in front of me to await boarding. In both instances there was plenty of space to maintain at least 6ft of distancing, but neither person was aware enough to realize the situation.
TSA Checkpoint in Oakland, not a single passenger to be seen. TSA precheck was even closed in Oakland, though it was open (with 1 person) in Denver.
Waiting for the airport train at Denver International, people nicely spaced out, wearing masks.
Walking through Terminal C at Denver International, barely anybody around at 6pm on a Friday evening.
Southwest Airlines boarding process in Oakland, a mad rush to the podium as always (only 10 at a time), not much organization to the boarding process.
The
Flight
Now on to the fun chaos of boarding. Southwest is famous for their open seat policy, normally boarding in groups of 30 at a time, all crammed together in small lines. Now they are calling up 10 numbers at a time to allow people to spread out. The problem is, when they call those 10 numbers it’s a free for all, no organization, so of course everyone immediately rushes to the counter and stands right next to each other trying to be the first on. I simply stood back, let them crowd ahead and walked on once my group had thinned out. Boarding the plane you have to walk by/near people, there’s just no fix for this situation (wearing my N95 still). I chose a window seat about halfway through the plane, spread out from other passengers, right now there is plenty of space on many flights. But, of course, on my first flight someone came and sat right in front of me (there was no need), so I moved over two seats to the aisle. As planes begin to fill up more and more the actual seating part is going to become impossible to not have several people within a 6ft radius of you, so that’s a part of travel risk one will just have to accept as being unavoidable. On the plane almost everyone was wearing masks, including the crew. But not long after take off many people removed their masks for most of the flight (about ½ on my first plane, and 10-20% on my second). I even witnessed one woman call the flight attendant over to ask a question, then promptly pull down her mask to speak directly with her (really???). On the flight I spent most of my time working and reading as I watched the scenery go by. I did sanitize my hands and remove my mask for a brief few seconds to grab a drink of water, but that was the only time in the 2.5h flight my N95 came off. Overall a pretty uneventful flight once we were in the air, no food and beverage service, a few trash collection passes by the friendly flight attendants, but that was it. Both flights landed early so we had to wait a few extra minutes for our gates. Even though very few flights are running (<30-40/day outbound at DIA and Oakland it looked like) each airport is only operating a fraction of it’s gates. When we finally got to the gate and the captain turned off the seat belt sign, the mad rush to the aisles to be the first off was on. Social distancing be damned, everyone did their normal thing and crammed into the aisle way right next to each other. So I simply stayed in my seat at the window, let most of the people deplaned, then grabbed my bag and headed out. I cleaned off my hands, took off my outer jacket and headed to the curb side. Again both airports were fairly empty for now, and getting through was a breeze.
On board headed to Oakland, most people spread out. After all, there’s only 20 of us. Masks still on.
Headed back to Denver, a few more people, but still everyone has their own row and plenty of space. Imagine this plane 2/3 full, with only middle seats empty. People in front and behind you, people across the aisle from you, etc.
People can’t help their natural tendencies. As soon as we land, it’s a rush to the aisle, everyone lines up nice and close to each other to rush off the plane.
Final
Thoughts
Right now the overall take home from my experience is that airports are fairly empty and the airlines are still trying to figure out how to manage travel during the Covid-19 pandemic (which will continue on for many more months ahead). While I was able to protect myself fairly well throughout the entire travel process, it was evident to me that one can not rely on the airline’s good intentions or the unaware strangers around you to protect you. And while right now it’s easy to find some space, once passengers start returning to air travel (and they will) you will be forced into closer quarters/contact with people no matter how hard you try to avoid it. Lines for buses, security, trains, escalators, seating areas at gates and on planes will all become busier to the point where you’ll have to be within 6ft of people, some will wear masks, some won’t (unless it becomes a Nationally enforceable law, unlikely). So if you choose to travel by plane in the next few months be prepared to accept the risk you are taking and knowing that you will be exposing yourself to people outside your realm of control and to people who might not all be acting very conservatively (or even think the virus is real). Hopefully during this lull in travel the airports and airlines can better test and implement their policies (I’ve written to Southwest), but that remains to be seen. And for those wondering, I’m now on a 14 day quaratine/watch for any symptoms (5/21, Day 3, ending 6/1).
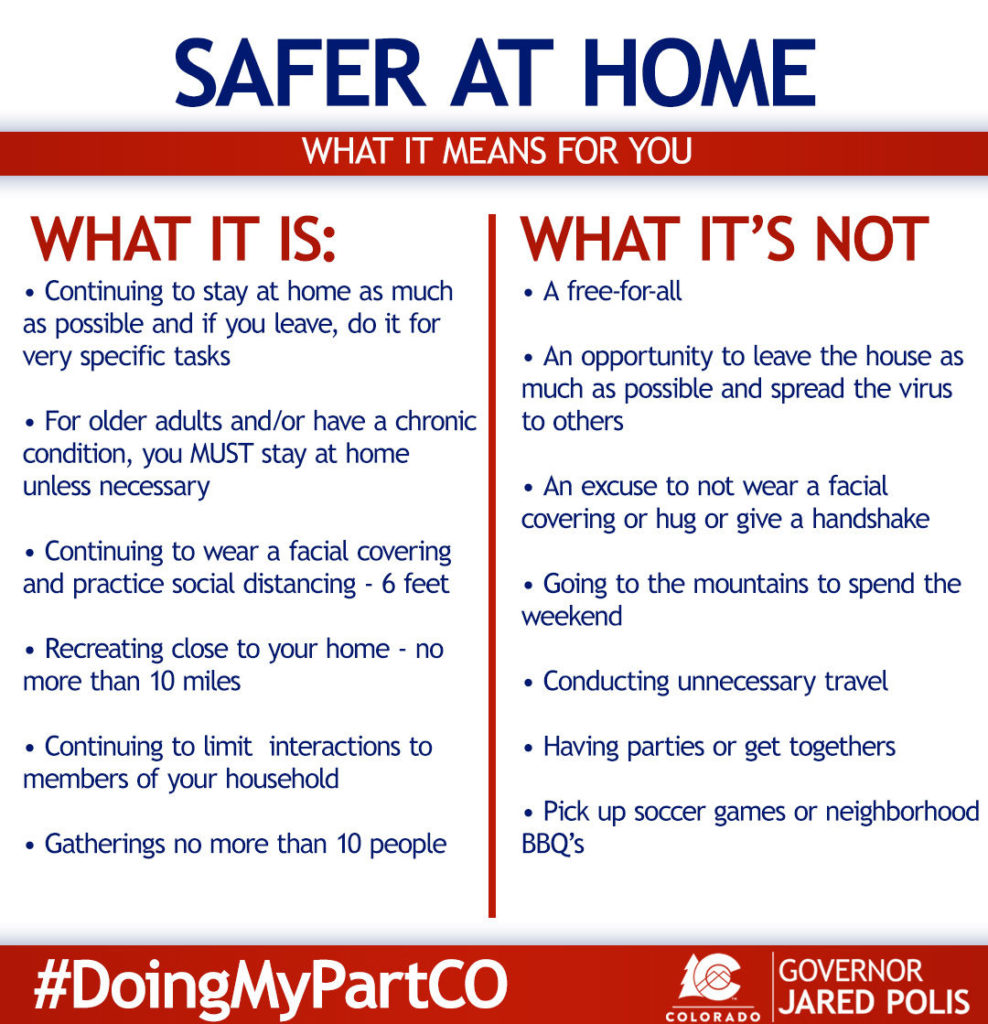
This past weekend much of the State of Colorado moved from “Stay-at-Home” to “Safer-at-Home” restrictions. This is the first step to us opening up more businesses and moving slowly back towards a state of ‘new’ normal. As part of this a lot of people across the country are preparing to go back to work (or into an office/store) in some capacity in the coming weeks. Some people think this is all BS and a hoax, you can stop reading now, for those who are worried or uncertain exactly what this return to a ‘normal workplace’ might look like, I’ll try to outline a few best practices that my work has been using and also highlight what the State of Colorado has outlined for businesses that are reopening.
Governor Polis’s outlines what Safer-at-Home means for Colorado. Note that individual Counties may enact additional legislation beyond these basic measures. Here in Boulder County masks are required in public settings where you can not maintain 6ft of separation.
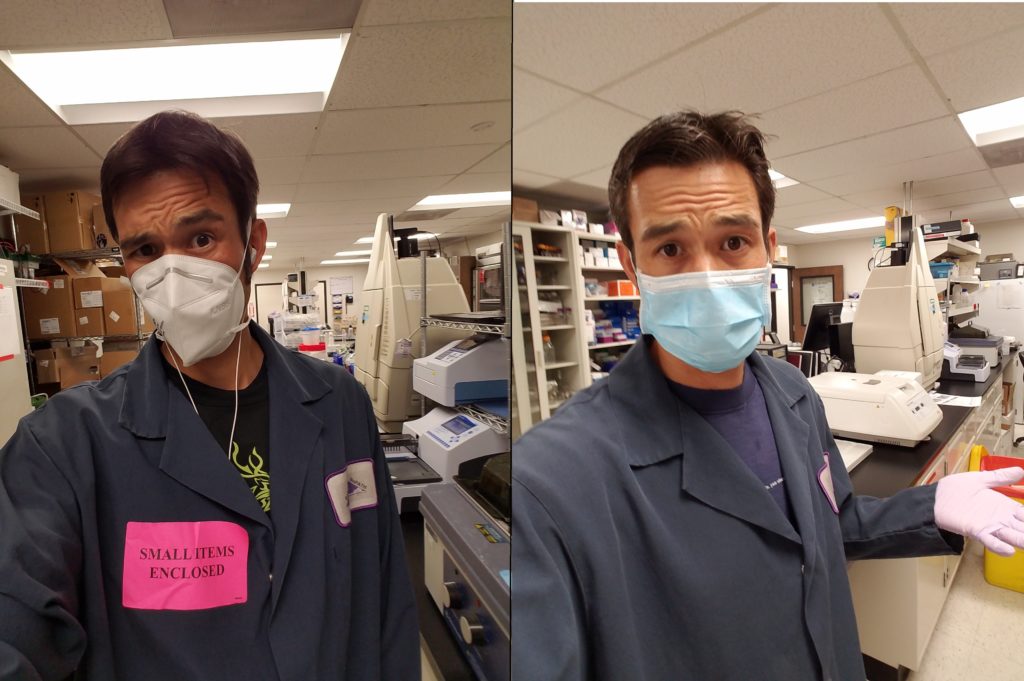
To start with for those that don’t know my background, I work in a vaccine and drug development laboratory. So my workplace will definitely look different than many of yours, but there are still many applicable practices that we’ve implemented that all types of work environments can utilize. Much of my experience in mitigating infectious hazards comes from years of working in Biosafety Level 3 facilities (with airborne, highly infectious, incurable pathogens). The stringent types of biosafety measures we implement in the lab aren’t applicable to daily life, except if you’re working in a healthcare setting in close contact with highly infectious patients (ping me separately if this is of interest to you). I’ll divide the topics up into three categories; general work place practices that should be implemented at the management level, engineering controls (equipment) and lastly how many of the common workplace practices can and should change to help you protect yourself during this uncertain time.
General
Workplace Policy
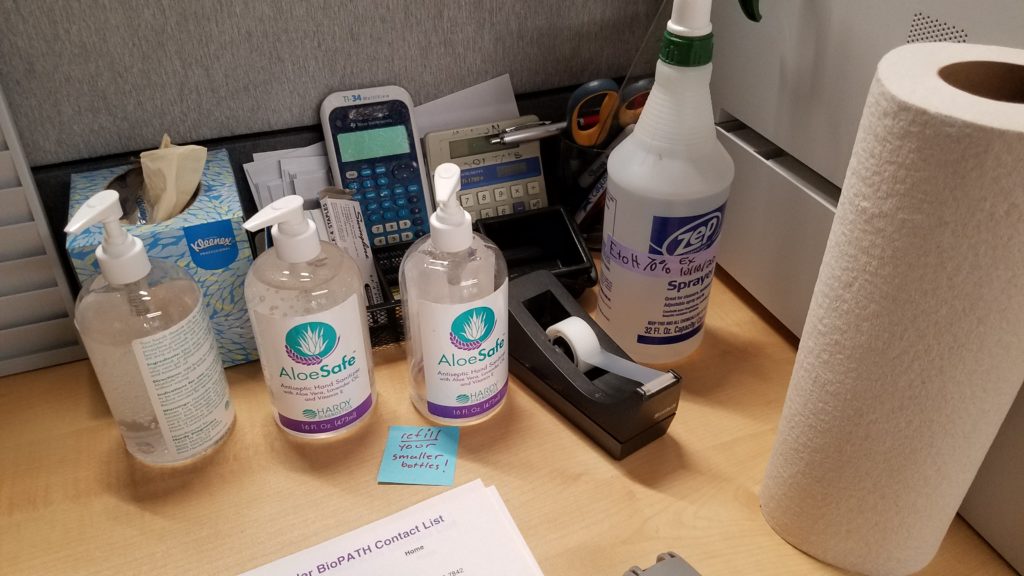
While some people can work remotely from home (best practice), many of us require specialized equipment/facilities, customer interactions or other tools that are simply not available at home. If your work place is welcoming employees back into the office/store, the State of Colorado has set out several guidelines for how work place policy should be setup to protect the employees. First, spread out the hours people work; work from home, work shifts, segregate tasks people are working on to different areas, etc. Second, the employer should be providing ample cleaning supplies, hand sanitizer and soap. In our office we also have an employee tasked with daily cleaning of the common areas and commonly touched surfaces (door knobs, time clock, fridge, conference table, etc). In addition to this I clean my personal desk each morning, it only takes a few minutes, but alleviates any concern about contamination of my immediate workspace. Third, the wearing of masks should be made mandatory for all employees (and customers) when you’re interacting with anybody else (even in passing or in the bathrooms) or moving around the office. The reason this needs to be made a company wide policy is, otherwise it’s too easy for a portion of the population to not adhere, making the effectiveness of cloth/surgical masks far less on a company wide scale, everybody needs to protect everybody else. Additionally, signage reminding everybody about the policies on staying home if you’re sick, hand washing, cleaning of common areas and wearing of masks are helpful. Many of these measures are requirements of the State of Colorado for reopening a business, check with your individual state about their requirements.
Mandatory cleaning supplies near our front entry. All offices should have these available for employee use.
Masks, gloves and all the protective equipment. Despite what Trump recommends, injecting bleach and UV irradiating yourself are not a good idea. But these are good tools for cleaning equipment and surfaces (just not your body).
Engineering
Controls
Engineering controls is a term used for physical barriers or equipment that is used to reduce the hazards of a workplace. In regards to COVID-19 in the workplace it’s referring to barriers and office setup that can help reduce interactions with coworkers and thus reduce the risk of someone getting sick. One method of limiting the workplace risk is to spread out employees desks/work spaces. Providing all employees with at least 6ft of space as to reduce the likelihood of infectious transmission. Another way is to setup barriers between employees desks/work spaces. This can be done by putting up plexiglass walls (or other materials) to block the direct line of transmission from one person to the next. So the open workspace system that so many tech companies love, is probably going to need to go away for the immediate future. Cubicles (or closed offices) actually provide a fairly safe way for each employee to have their own protected space, where infection risk is low, and you don’t have to wear a mask all the time. Work with your employer to establish these ‘safe zones’, because not only will it reduce the transmission risk, but it makes the employee far less anxious because they have their own personal space (at least in our office it works that way). For those of you working retail, store fronts or other customer based jobs, many of these rules won’t directly apply. My recommendation would be to establish a safe zone for yourself (back room, office, car, outside). Take breaks to get out of the mask for a few minutes (pretend like you’re a smoker) or just to step into the back room/warehouse for a few minutes to relax and breath. Plan and prepare for the long haul.
The dreaded cube farm, a great way for every employee to have their own protected safe space and to minimize COVID-19 transmission risk.
Common
Workplace Practices
While the previous two sections mostly addressed changes that can/should be broadly implemented in the workplace, this section is going to address how the actions of individuals/groups should change. I have a feeling for many people this is going to be the hardest section to incorporate into our daily lives, but these changes are equally as important as those above. The first one is simply an extension of the general social distancing policy that pervades our lives, but applied to the workplace. No group lunches, standing around the coffee/espresso machine, office parties, etc (yes, sad face, I know). It doesn’t mean you can’t chat with coworkers or socialize, but it does mean it has to be done at a safe distance apart and while wearing your masks. If/when you need to use common office equipment (printers, coffee makers, fridge, cash register, etc) either make sure the equipment is well cleaned off or sanitizer/wash your hands afterwards as a precaution. This mitigation measure may be slightly less important for some workplaces, and more important for others (depending on how many people you’re sharing space with). On the far end of the spectrum are people whose jobs require direct contact with others (massage therapist, physical therapist, hair stylist, acupuncturist). For these professions it’s even more important to sanitize all surfaces after each client, wear masks (tough for hair salons), make sure both client and provider clean their hands before interacting, and of course pre-screen your clients to make sure they are not sick or symptomatic.
The last one
is probably fairly obvious for many people, but meetings are going to look quite
a bit different (if they happen at all). The easiest way to mitigate the risk
is to do virtual meetings (Zoom, Skype, Teams, etc) whenever possible. Of
course sometimes it’s much faster and more efficient to meet in person, which can
definitely be done very safely. The smaller the better to start with, but as meetings
grow, ensure there is at least one seat between everybody in the room, and
everybody continues to wear their masks when in the same room.
Workplace meetings in the COVID-19 era. Join virtually, space out, masks for all those who attend in person.
Final
Thoughts
My office/lab implemented most of these procedures the first week of Colorado’s Stay at Home order and shutdown. We have our own cubicles/workspaces that are our own private areas when we’re not working in the common lab spaces. We wear gloves (because it’s a lab) and masks whenever working in close proximity to others, common surfaces are regularly cleaned, our employees with COVID-19 risk factors spend much of their time working from home, or working off shifts, our meetings are done half virtual half in person (with masks). Using all these measures we’ve had no issues with viral transmission and also minimal issues slowing down our workflow. If you or your employer are hesitant to implement many of these actions, just look at the extreme cases of the meat packing plants all over the country. They stayed open but didn’t implement any infection risk mitigation (employees working in close quarters), and ended up suffering large outbreaks forcing their businesses to shutdown. So it’s really in everybody’s best interest to protect themselves and those around them, to stay healthy and keep the business running without the major setbacks that an outbreak would cause.
While company wide policy is up to the employer, you are your own strongest advocate. So it’s important to assess your work place (and how it operates) and how best to mitigate risks. If an employer isn’t providing you at least the minimum levels of protection outlined above, then speak with your local public health department, as they will come in and further assess what more can and should be done. Going back to work in and of itself isn’t a problem, it’s doing so in a responsible and controlled manner that allows your workplace to implement and test out these new policies. For all businesses there will be a trial period of adjustment to the new way of functioning, just be flexible and understand most of these changes really don’t dramatically affect our lives (and definitely don’t impinge our our civil liberties), we’re all going to get through this.
Sorry for
the delay, but this one has taken a lot of time and thought to put together
(and reading some 80 odd Covid research papers). My goal in this edition of
Covid Science Theater 2020 is to talk about what happens when the virus enters
our body, infects our cells and subsequently leads to either mild disease or
more severe infections. It’s going to be a fairly dense article, but I’ll do my
best to keep the science and terminology to something generally understandable and
hopefully educational.
For those who don’t want to delve too much into the specifics of all the virology, immunology and pathology I’ll provide a short 1 paragraph set of clifs notes here. The virus most commonly enters the host through mucus membranes (eyes, nose, mouth) and infects vascular endothelial cells and cells of the lungs, kidneys, GI tract and begins to replicate. The body initially responds to the virus through a host of Innate Immune mechanisms; these generic counter measures are deployed against all invading pathogens as a first line defense and are not specific to the invading pathogen. Unfortunately, these initial immune responses aren’t always adequate to contain the virus (the virus sometimes evades destruction, other times the virus just overpowers the immune response) so our body deploys a second type of response known as the Adaptive Immune response. In this phase, T-cells and B-cells are primed to respond to the specific infectious agent (here, SARS-CoV-2). Often this two-pronged approach works to contain the infection, eliminate the virus and build up lasting memory to subsequent infections. Unfortunately in some people the virus spreads too rapidly and the immune response doesn’t respond appropriately, leading to destruction of their organs (notably the lungs) and potentially death. Sometimes this more severe outcome is caused by the virus itself, but more often it seems to be caused by an overzealous immune system trying to play catch-up. So there’s the quick and dirty; in the following paragraphs I’ll go into more detail about Viral Entry/Binding/Replication, Early Cellular Responses, Clinical Symptoms, Adaptive Immune Response and What Happens and Why the Immune System Sometimes Fails.
The information in the following paragraphs comes from a combination of basic immunology principles (Kuby Immunology textbook), observations and early research released about Covid-19 and conclusions drawn from earlier studies of SARS-CoV-1 (a virus that is very similar to the current SARS-CoV-2, but with some caveats of course). As Covid-19 is still a new disease, we are constantly learning new things about the virus, infection cycle and pathology, so while what I outline here is based on a lot of research, there are definitely aspects of this virus that we don’t fully understand, and need further investigation.
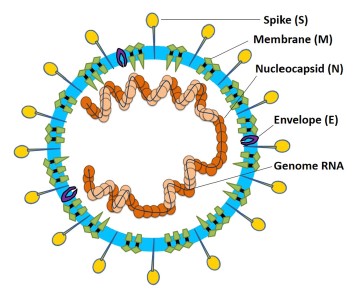
Graphic of the structure of a SARS virus, the S, M and E proteins are the most important in regards to host recognition, Li et al 2020.
Viral Entry and Replication
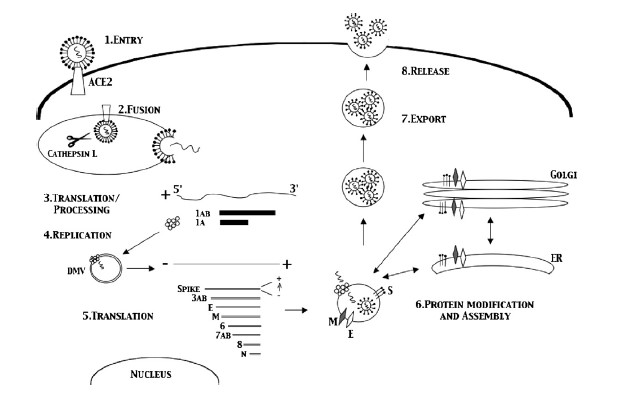
Coronaviruses get their name from the hallmark shape, a circular capsid (or shell) that is spiked with proteins on the outside and sheltering the virus genetic sequence on the inside. The Spike (S), Membrane (M) and Envelope (E) proteins make up the majority of the viruses outer shell, while the Nucleocapsid (N) protein found inside the virus assists in viral replication. This small assortment of proteins, plus a few others, make up the bulk of the very simple viral structure (Weiss 2005, Li 2020). The novel coronavirus 2019 (COVID-19) shares a lot of homology or similarity with the original SARS virus that was discovered in 2002, genetically 80% similar, while being 76-95% similar for the major proteins listed above (Xu 2020). This allows researchers to draw a lot of conclusions from previous research on SARS-CoV-1, though we must be careful when doing so, as there are some known (and unknown) differences between the two viruses. The infection cycle starts with the virus gaining entry to the host, usually through mucus membranes of the eyes, nose and mouth. Once inside the virus often begins it’s infectious cycle by infecting vascular endothelial cells that line vessels throughout the body. While different viruses have different mechanisms by which they enter host cells, SARS-CoV-2 binds to the ACE2 receptor using its spike protein (same as SARS-CoV-1), allowing it to enter the host cell (Jia 2005, Walls 2020). Like most viruses, SARS-CoV-2 then goes through a multi-stage process by which it hijacks some of machinery inside our own cells to in order to replicate, escape and subsequently infect more cells in a continual cycle (Frieman 2008).
Overview of the SARS viral life cycle inside the host, Frieman et al 2008.
Early Cellular
Response
Thankfully our body has a whole host of immune mechanisms it utilizes to deal with infectious agents of all types. Almost as soon as an invading pathogen has infected our cells the immune system starts going to work. The Innate Immune response is our constantly active sentinel, whose cells are constantly circulating all over our body just looking for foreign invaders to attack and kill. These innate cells use Pathogen Associated Molecular Patterns (PAMPs), or markers of foreign invaders, as the initial signals something is wrong and that it’s time to go to work (Li 2020). Some cells go to work directly attacking the virus and infected cells in an attempt to destroy the virus, others release signaling molecules known as cytokines and chemokines that recruit other cells to help in the fight (Frieman 2008), and some cells just go ahead and sacrifice themselves in an effort to prevent the virus from hijacking them, a process known as apoptosis (Lim 2016).
Symptoms:
What and How They Manifest
While this system works well for many invading pathogens (why we are not sick all the time), allowing our body to control the infection, many viruses (and bacteria) have evolved mechanisms by which to evade, subvert and co-opt the immune response to their advantage. For SARS-CoV-2 it seems to be able to prevent the host immune system from activating one of it’s key anti-viral signaling pathways, the Type 1 Interferon pathway (Lim 2016, Li 2020, Frieman 2008). While it is not known exactly how the virus subverts this system a few hypotheses involve the Nucleocapsid protein (Lim 2016), other non-structural proteins (Lim 2016), and some of the SARS enzymes (Chen 2014). So by reducing the host immune response the virus is able to more effectively replicate and spread, leading to a more systemic infection. This is when we start to experience more of the hallmark symptoms of the infection; fever, sore throat, coughing, fatigue, pulmonary inflammation leading to shortness of breath and possible pneumonia and lymphopenia (a decrease in lymphocytes, more on that later) (Huang 2020, Zhu 2020). Most of these symptoms are a physical outcome of the body’s ongoing fight with the virus, trying to delicately balance destroying the invader, while preserving the host organs and system. The fever is the immune system’s attempt to raise the core temperature enough to burn out the infection. The sore throat/cough is an outcome of our immune system attacking infected cells of the airways and trying to expel the invader (mmm mucus), same for the pulmonary issues (initially, more on this later too). While many of these symptoms may be scary and uncomfortable they are often a normal part of our body’s healing process when dealing with a foreign invader. So under normal circumstances, it’s best to rest and let your body do it’s thing, unfortunately this doesn’t always go as planned, as we’ll find out in the following sections….
Adaptive
Immune Response; Stage 2
In the previous two sections you’ve seen how our well intentioned Innate Immune system can sometimes fail leading to illness, thankfully the body has a backup, the Adaptive Immune response. This secondary wave of the immune response goes into action very soon after the initial infection (several hours to few days, infection dependent) and is mostly comprised of two cell types; T-cells and B-cells. When the levels of virus in the body start to rise, several of the innate immune cells can act as activators of the adaptive immune response, taking pieces of the virus to specialized activation centers know as lymphoid organs. These centers of immune activation are spread all over our body and are the primary site of pathogen specific antigen (virus pieces) presentation. The antigen presenting cells (Dendritic cells are most prominent) present the virus to the T-cells and B-cells as if locks in a door, allowing the T-cells and B-cells to go to work making specific keys (receptors and antibodies) that can attack and destroy the pathogen in a very focused manner. The outer proteins that make up the viral capid (proteins S, M, E) tend to be the most effective as this is what is visible to our body when intact virion are released (Liu 2017). So the body makes a whole army of these specific cells that traffic to the sites of infection; T-cells directly attack the virus and infected cells, while B-cells make antibodies that bind to parts of the virus, preventing them from entering new cells and marking them for destruction (Liu 2017).
These two arms of the Adaptive Immune response are also what comprise our immunological memory. Virus specific T-cells and antibody producing B-cells remain dormant in specialized lymphoid organs (sometimes they also remain in circulation), just waiting for the virus to turn up a second time. This time since they are already primed and ready to go, memory T-cells and B-cells start attacking the virus almost immediately, usually preventing the virus from spreading and preventing us from getting sick. Studies of SARS-CoV-1 have found both memory T-cells and memory B-cells (producing neutralizing antibodies) that are capable of rapidly responding to viral reinfection (Li 2020, Liu 2017, Channappanavar 2014). In human patients who recovered from SARS-CoV-1 infection anti-SARS antibodies and memory T-cells were found in most patients up to 24 months after infection (Liu 2006, Ka fai 2008, Liu 2017). While antibody responses did decline over time in SARS-CoV-1 patients (many undetectable at 6 years), memory T-cell responses were conserved for up to 11 years after infection (Tang 2011, Ng 2016, Liu 2017). Similar high quality neutralizing antibodies have been found in COVID-19 patients, but since the disease is so new the longevity of memory responses to this new virus aren’t exactly known. Encouragingly, since SARS-CoV-2 is so similar to the original SARS virus, and lab testing has even shown that their be might cross-reactive protection between the two diseases (Walls 2020), there is much hope that the long lasting memory responses seen for SARS-CoV-1 would also apply to those who have recovered from COVID-19. All of this evidence, both old and new, does inspire a lot of hope that a functional vaccine would both be likely and very effective in providing some duration of immunity from COVID-19, but how long remains to be seen.
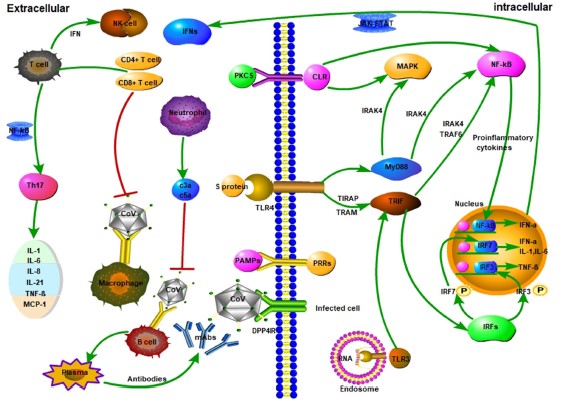
Graphical overview of the many cells and pathways involved in the host immune response to SARS. It’s a complex set of feedback loops and interactions with a lot of variables. Li et al 2020.
When the
Immune System Fails, Severe Disease
The reason COVID-19 is such a scary disease, isn’t because our immune system has no problem fighting it off, but because in some percentage of the cases (uncertain, but estimates are as high as 10-20%) patients need to be hospitalized due to severe complications. If our immune system is so complex and so strong, why do patients with COVID-19 get so sick that they need hospital care? It comes down to numerous very subtle things this virus does that are different than coronaviruses that cause the common cold. One is the effect SARS-CoV-2 has on Type 1 Interferons mentioned earlier, reducing the body’s initial response to infection. Another early symptom seen in many severe cases is lymphopenia, or a loss of lymphocytes (notably T-cells) early on in disease (Huang 2020, Schmidt 2005, Weiss 2005). While the exact cause of this loss of T-cells is not known, it is hypothesized that the viral proteins may lead directly to T-cell death as a mechanism of immune evasion (Lim 2016, Li 2020). These mechanisms of avoiding immune detection along with the efficiency of viral replication can lead to an out of control infection very quickly.
But in the end, it’s only partially about the virus, and largely about an overexuberate immune response. In an attempt to catch-up to the wide-spread infection the immune response goes into overdrive, ramping up a lot of the inflammatory cells and signaling molecules that tell the body to attack the infection (Li 2020). This response does in fact kill the infected cells, but it also destroys lung tissue (primary target), vascular tissue, liver tissue and other infected tissues (Tian 2020, Schmidt 2005). This is often when the more obvious signs of pneumonia set in; the lungs fill with fluid, the efficiency of aveoli decreases (oxygen absorption) and breathing becomes very labored and difficult. This is the tricky thing about COVID-19, making our immune response more efficient would help prevent early infection, but later on would lead to increased tissue damage. But if we reduce the immune function of the body to prevent self-inflicted tissue destruction, we run the risk of allowing the virus to run rampant throughout our body. COVID-19 is a tricky disease to treat for these reasons, and because the disease severity has a wide range of outcomes for different people. In some, infection is very mild and asymptomatic, in others, their entire body shuts down as the virus (and immune system) destroys the host from the inside. The reason many comorbidities are important as risk factors for severe disease is that most of them either affect the immune system or lung function. Obesity, diabetes, auto-immune diseases all alter the immune system’s ability to function, making it harder to fight off the virus. COPD and asthma (though less prominent then thought) make the host pulmonary system more sensitive to damage caused by the virus and immune system.
But not all hope is lost! Because of the large body of evidence suggesting that SARS viruses create robust lasting immunity, this means a vaccine might be very effective at protecting most of the population. Also, now that there are many patients who have recovered from COVID-19, tests are underway to examine if using their plasma (containing antibodies) can help patients who are suffering from more severe cases of the disease (works for other viruses like Ebola). We also have several promising anti-viral agents that are already in clinical trials being tested against COVID-19, with hopes that one or more of them will help improve patient outcomes and be ready for use later this year. Unfortunately all of this does take time, meaning we won’t have a cure next month, but by slowing the spread of the virus, not only do we allow hospitals to manage the patient load, but we allow all the scientist out there to catch-up and produce much needed data, therapies and vaccines.
Thanks for reading. If you see any mistakes please bring them to my attention and I will correct them ASAP. If you have additional questions or want to discuss the immune response in more detail (this is a very high level overview) I’d be happy to do so via text or email. Stay safe and stay healthy.
Literature Citations: Chan et al, Serological Responses in Patients with Severe Acute Respiratory Syndrome Coronavirus Infection and Cross Reactivity with Human Coronaviruses 229E, OC43, NL63. Nov 2005, Clinical and Diagnostic Laboratory Immunology. Channappanavar et al, T cell-mediated immune response to respiratory coronaviruses. May 2014, Immunology Res. Chen et al, SARS coronavirus papain-like protease inhibits the type 1 interferon signalling pathway through interaction with the STING-TRAF-3 TBK1 complex. Jan 2014, Protein Cell. Frieman et al, SARS Coronavirus and innate immunity. 2008, Virus Research. Huang et al, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Jan 2020, Lancet. Jia et al, ACE2 Receptor Expression and Severe Acute Respiratory Syndrome Coronavirus Infection Depend on Different Human Airway Epithelia. Dec 2005, Journal of Virology. Ka-fai Li et al. T cell responses to Whole SARS Coronavirus in Humans. Oct 2008, Journal Immunology. Li et al. Coronavirus infections and immune responses. Jan 2020, Journal of Medical Virology. Lim et al. Human Coronaviruses: A Review of Virus-Host Interactions. 2016, Diseases. Lu et al. Immune responses against severe acute respiratory syndrome coronavirus induced by virus-like particles in mice. June 2007, Immunology. Ng et al, Memory T cell responses targeting the SARS Coronavirus persist up to 11 years post-infection. March 2016, Vaccine. Schmidt et al. Coronaviruses with a special emphasis on First Insights Concerning SARS. 2005, Birkhauser Advances in Infectious Diseases. Tang et al, Lack of Peripheral Memory B cell responses in Recovered Patients with Severe Acute Respiratory Syndrome: A Six-year Follow-up Study. May 2011, Journal of Immunology. Tian et al, Pulmonary Pathology of Early-Phase 2019 Novel Coronavirus (COVID-19) Pneumonia in Two Patients with Lung Cancer. Feb 2020, Journal of Thoracic Oncology. Walls et al, Structure, Function and Antigenicity of SARS-CoV-2 Spike Glycoprotein. Apr 2020, Cell. Weiss et al, Coronavirus Pathogensis and the Emerging Pathogen Severe Acute Respiratory Syndrome Coronavirus. Dec 2005, Microbiology and Molecular Biology Reviews. Xu et al, Systematic Comparison of Two Animal-to-Human Transmitted Human Coronaviruses: SARS-CoV-2 and SARS-CoV. Feb 2020, Viruses. Zhou et al, Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. March 2020, Lancet.
There’s
been a lot of debate and misinformation floating around about the use of masks
for the general public as a measure to prevent the spread of infectious
diseases, specifically Covid-19 in the United States. Do they help, do they
not? Is an N95 really better than a surgical mask, is this better than a cloth
mask? How and when should they be used? On 4/3/20 the CDC in the United States finally
came out with a blanket recommendation that ALL citizens of the United States
wear some sort of face covering whenever in public. This was a dramatic change
of direction from the previous recommendation that masks were completely unnecessary,
except for front line hospital workers and for the infected. In this rendition
of Eric’s Science Corner I’ll do my best to present some of the data and
studies that have looked at the questions above, in an attempt to clarify the
misunderstandings and the mixed messages. The topics I’ll try and cover are;
what are the different types of masks and what are they designed to do? How useful
are the different types of masks for the general public? And finally, a few
best practices on how to wear and use a mask or face covering. Rule #1, just
ignore anything Donald Trump says, now on with the info.
Defining
Mask Types
To start
there are three main categories of face masks that I’ll be discussing; fitted
N95 respirators, professional grade surgical masks and cloth masks (variety of
materials). There are numerous sub-categories for each and also other types of
protective face wear I won’t discuss because they aren’t really relevant to the
general population, only to those in the hospitals and those of us who work in
laboratories. The first type is the fitted N95 respirator, these are face
fitted respirator masks that have been certified to filter out approximately
95% of aerosols and particulate matter (when worn properly). You breath through
either a small filtration unit in the front of the mask or directly through the
filtering material of the mask, NOT around the sides (as it should be sealed).
The professional grade surgical masks that many of us have seen in the
hospitals are loose fitting non-sealed masks that are designed to block the
wearer from inhaling large droplets/splashes and to block their respiratory emissions
(protecting others around them). They are not designed to prevent the wearer
from inhaling aerosolized particles as they are not sealed around the edges
(cdc.gov, crosstex.com). The final group are the cloth masks which can be made
from various materials. Their main purpose is to allow more comfortable
widespread facial covering for the general public; to reduce the inhalation of larger
droplets and to reduce one’s own exhalation and aerosol creation. These types
of masks are not specifically certified in any way, though I will discuss the research
that has been done looking at filtration, efficacy and utility of the different
materials.
On the left is a standard N95 Respirator mask, on the right is a surgical mask.
So now on
to how well do these different types filter out microparticles, specifically in
regards to viral transmission (because that’s what’s on everyone’s mind). Numerous
studies that compare N95s and surgical masks and how they prevent infection in
hospital settings have shown both to be similarly effective when dealing with droplet
based respiratory viruses like influenza (Randanovich 2016, Smith 2016). Laboratory
testing of these two types of masks does confirm that the smaller the particle
size, the better an N95 performs compared to a surgical mask (van der Sande
2008, Shakya 2016), thus they are more effective for those dealing with high
level risk of aerosolized viral exposure. These two types of masks are
certified, so it’s no surprise they perform fairly well, but what about the
cloth and homemade masks? The first thing to consider is the type and thickness
of material being use for the mask. Things that allow easy breathing or light
to penetrate aren’t going to filter the air as efficiently, but if it’s too thick
that you can’t breathe through it then it becomes extremely hot, uncomfortable
and unwearable (and you breath around the sides, rather than through the
material). One study comparing the filtration efficiency (of masks in a lab test,
not on a person) of different materials found that items such as tea towels and
cotton mixed fabrics did the best job of filtering particulate matter (up to 70%
mean filtration) out of the air, while silk, scarves (like buffs), pillow cases
and normal cotton T-shirts did not perform as well (45-60% mean filtration efficiency),
with surgical masks being their standard (90-96% mean filtration) (Davies 2013). When commercially available cloth
masks were compared to surgical masks on humans (again in a lab) filtration
efficiency was more variable; with cloth filtering out 30-50% of microparticles
while surgical masks filtering out 60-90% of microparticles and N95s
consistently filtering out 80-95% (Shakya 2016). The efficiency of filtration
directly correlated to the size of the particle, with cloth masks performing
the poorest on particles small than 1µm in size. So that’s a little background
about how the masks are INTENDED to be used and how they function in a
laboratory, how about in real life?
Use in
the General Public
By now you’ve
probably heard many times that the public should not hoard or use N95s because
we need them for our frontline workers (very true) and they don’t work for the
public (partially true). The first piece is that because of the size of this
pandemic we don’t have sufficient supplies of N95s for highly trained hospital workers
who are coming into direct contact with the virus on a daily basis, thus need
this heightened level of protection, first (and most important) reason not to
stock up or hoard them. The second is that for an N95 to be at it’s most useful
and functional you have to have it fit tested, you need to be trained in proper
techniques to don/doff a mask and you have to actually use it correctly (you
can’t be taking it off to talk, to eat, to drink, basically you can’t break the
seal unless in a clean contained environment). They are also designed to be
disposable, meaning you can’t wash them, though sadly our healthcare workers
are being forced into extreme measures to try and sterilize/reuse them for lack
of options. For the general public a surgical mask would be a descent option
because they are designed to reduce droplet transmissions and to block one’s exhalations
(protecting those around you), but sadly our hospitals are also short on these
too, so for now they need to be saved for the frontline works (and patients) where
they’ll do the most good. Also remember that both of these are designed to be
disposable, so can’t be washed and aren’t designed to be reused for weeks on
end (like the public would need).
So this brings
us to cloth masks and their use in the general public. Mistakenly the US government
(CDC) originally came out saying that cloth masks don’t work and that they aren’t
necessary. By now most people have realized this isn’t exactly true, because
why else would they change their minds and recommend people wear them? Yes,
cloth masks are NOT designed to stop all tiny viral particles (and aerosols)
from passing through, and yes they are not highly efficacious, but that doesn’t
mean they don’t help. While a cloth mask won’t fully stop one from inhaling aerosols
and microparticles, they do filter out some of the smaller aerosols (30nm-1µm)
but more importantly block larger droplet transmission both inward and outward
(Davies 2013, Shakya 2016). So while they do filter some of the air you’re
inhaling, the major benefit of a mask is to protect those around you by minimizing
the amount of aerosols you create. This is especially true with the knowledge
that those infected with COVID-19 can be asymptomatic but still capable of
spreading the infection. For masks to be most beneficial we all should wear
them in any public setting where we’ll be interacting with others (even if we’re
socially distancing).
Best
Practices for Masks
Now on to a few personal suggestions for best practices when using a face mask. Note that much of this stems from my own personal training having worked in Biosafety Level 3 laboratories (blood and aerosol transmitted infectious diseases) and in hospitals, but some additional guidance can be found on the CDC website (CDC.gov). First off, once you’ve made/acquired your mask, put it on at home and work on the fit, comfort, breathability. A mask that doesn’t stay on or that you can’t semi-comfortably wear (to the point you’ll touch it a lot or take it off) isn’t very useful. Look to make sure it fully covers your nose and mouth, has a pretty good fit around the bridge of your nose and the sides, and that it won’t slip down when you turn/move your head.
Once you’ve
established it works, wear it around for 20-30min inside your house to get used
to the idea of breathing through a mask. It’s probably going to be a bit awkward
at first, as for most people they’ve never had to do it before. This exercise
will make it easier to wear in public without thinking about it too much. Now
on to that more critical step, wearing it out. The main times the mask should
be worn is whenever you’re going into a public area where you might have close contact
with others. If you’re just sitting in your car and driving around, no need to
wear a mask, but if you go to the grocery store, pharmacy, liquor store, gas
station, work, or even walk around your neighborhood it’s best to wear the mask
to protect those around you, even if you don’t think you’re sick.
To put on the mask, do so BEFORE entering that public space, meaning your home entry if you’re walking around the neighborhood or inside your car before you walk into a shop. Then clean your hands off so that you are less likely to contaminate other surfaces (hand sanitizer or washing). When you’re wearing you mask you SHOULD NOT be taking it off or moving it off your nose/mouth until you’re back in your non-public safe area. Wearing it half the time, pulling it down half the time, taking a break to eat or drink in public negates some of the benefits and protection and also adds to the chance that anything you pickup on your hands will be transferred to your face. When you’ve exited the public space, wash/clean your hands then grab the strings/band of the mask and remove it (do not grab the front of the mask itself). If you have a washable reusable mask proceed to wash it with soap and water. Disposable masks are supposed to be discarded into the trash (hence why not ideal for daily use in public). While your mask is your barrier of protection, remember it’s not foolproof, and is merely a way to further reduce your risk of becoming infected and infecting others. IT DOES NOT change the fact we should be social distancing and providing each other space or that we should be staying at/near home and avoiding any unnecessary travel/errands. Wearing a mask is just another tool in our arsenal to help slow the spread of the virus and reduce transmission rates.
One last note about gloves. Wearing gloves for most people in a public setting is useless (yes I said useless). Gloves are a very effective piece of PPE for trained healthcare and lab workers, but in our daily lives most people treat gloves just like their normal hands. They touch common surfaces, pick up food items, open doors, text on their cell phone, touch their mask, etc. All of these practices together make the use of gloves just as bad as dirty naked hands. You’re better off just considering your hands as dirty whenever you’re in public and not touching any of your personal belongings (including that cell phone) until you’ve cleaned them. If you have to touch your phone or food items while in public, there are many ways to also clean these surfaces as well. Don’t waste gloves and don’t touch your face.
Citations Balazy et al. Do N95s respirators provide 95% protection level against airborne viruses, and how adequate are surgical masks. American Journal of Infectious Control, 2006. cdc.gov/hai/pdfs/ppe/ppeslides6-29-04.pdf . CDC Guidelines for Selection of PPE in Healthcare. cdc.gov/niosh/npptl/pdfs/UnderstandDifferenceInfographic-508.pdf . Understanding the Differences, Surgical Masks, N95 Repsirators. crosstex.com/sites/default/files/public/educational-resources/products-literature/guide20to20face20mask20selection20and20use20-202017.pdf . Guide to Face Mask Selection. Davies et al. Testing the Efficacy of Homemade Masks: Would They Protect in an Influenza Pandemic. Disaster Medicine and Public Health Awareness, 2013. osha.gov/Publications/osha3079.pdf . OSHA Respiratory Protection Guidelines. Randanonvich et al. N95 Respirators vs Surgical Masks for Preventing Influenza amount Healthcare Personnel. JAMA, 2019. Sande et al. Professional and Home-Made Face Masks Reduce Exposure to Respiratory Infections among the General Population. PLOS One, 2008. Shakya et al. Evaluating the Efficacy of Facemasks in Reducing Particulate Matter Exposure. Journal of Exposure Science and Environmental Epidemiology, 2016. Smith et al. Effectiveness of N95 Respirators vs Surgical Masks in protecting healthcare workers from acute respiratory infection: a systematic review and meta analysis. CMAJ, 2016.
It’s been a week since my first Covid-19 blog on 3/18/20, and I will have to admit how amazed I am at the feedback and attention it got. A LOT has happened since that day, and not all of it has not been so positive. Here in Colorado Governor Jared Polis officially announced today (3/25/20) that ALL residents of Colorado are under a ‘Stay at Home’ order. Meaning we’re supposed to stay in our place of residence with the exception of essential trips (medical, food, work for us exempt jobs) and exercise, all the while maintaining social distancing from anyone not in our immediate household (which is just me and my cat). For many of us this isn’t too much of a change, but for those who didn’t think this was serious it’s probably a bit of a rude awakening. Since my post LAST WEEK (now 3/26/20) the number of worldwide confirmed cases has more than doubled to 530,000 (from 219,243), the number of deaths has increased to over 24,000 (from 8,968) and on 3/26/20 the United States confirmed over 17,000 NEW cases, making us the country with the most confirmed cases in the world (go us?) (worldometers.com, washingtonpost.com).
I’m hoping by now that most people realize how serious this is, and that there is definite need to slow the spread; both to allow our medical care teams to keep up and to allow scientist to keep working (please no arguments on the political actions or economic impact, yes it’s going to be bad). My goal in this blog write up is to outline the things that help us bring this pandemic to an end (or at least slow it down). I’ll be focusing on the status of testing in the US (what those tests are), the current drug pipeline and what is being tested, the process and timeline for a vaccine and whether there’s anything to the claim of seasonality with the infection. So here we go, Round 2, diving back into the Science!
Testing
So in my last post I wrote about how much of a mess the Covid-19 testing and surveillance were in the United States, well sadly that has not improved a whole lot. While we’ve definitely tested a lot more people, I’ve been hearing from providers and hospitals all over the country that they’re only testing people who are in high risk populations or have advanced/severe cases of disease. Very recently a rash of new tests have become available to providers and hospitals, meaning the surveillance is starting to grow and hopefully this will continue. There is definitely hope as we are soon to have two different types of tests available, the PCR based tests that we’re currently using for diagnosing active disease and an Antibody based test.
The PCR based test is the one I spoke about previously where labs are able to look for pieces of the viral genome in human samples (usually a nasopharyngeal swab). This test can be quite sensitive and is used to identify infected patients even during the early stage of disease. Though, being such a sensitive test it is more prone to errors and false positives (though they are still very well validated), hence why the original CDC test failed. The other issue right now is that because there’s not a lot of top down coordination in the United States we have dozens of different labs who have created PCR based tests that are being used in different parts of the country. Here are a few of the companies/hospitals who have created PCR based tests; ThermoFisher, Roche, Cepheid, Mayo Clinic, Stanford University, University of Pittsburgh, Atrium Health and the list goes on and on. The CDC even setup a website to allow researchers to develop their own tests and to provide some general guidelines. While on the surface this seems smart, it also means we don’t have any national coordination in our Covid-19 testing on the ground.
The second type of test that is just now being release is a test to look for IgM and IgG antibodies in the blood of patients. You might remember in the previous post where I talked about us building immunity to the virus? Well, antibodies are one of the hallmarks of immunity, and we can test for them, even after we’re no longer infected. A simple prick of the finger (a little blood) on a indicator strip and we have a positive or negative for SARS-CoV-2 antibodies in minutes rather than hours or days, think of it like a pregnancy test for Coronavirus (United Biomedical, Aytu Bioscience). The problem with these tests is that SARS antibodies may not be detectable until 7-14 days after onset of symptoms (Chan et al 2005), so there’s a good chance they won’t identify people who are in the early stages of disease. They WILL help us dramatically as we attend to understand the true prevalence of the disease and how many people are now immune. Once a person is immune and recovered you’re very unlikely to pickup or spread the disease.
Drugs and Clinical Trials
Much to the chagrin of many of us in the biomedical research sciences and healthcare, Donald Trump touted hydroxychloronquine as a ‘game changer’….wow wow, let’s pump the breaks for a second, back it up, and talk about the process by which drugs are created, rigorously tested and finally produced for mass distribution (if they even make it there). The first step is identifying potential drugs and targets then testing them in a laboratory to see if they actually work like you hoped and they’re not excessively toxic. This usually involves some mix of cell culture and animals models. If a candidate is lucky enough to make it through the lab testing phase (known as pre-clinical trials, only 1 in 1000 do) then the company can apply to the FDA to move it’s drug on to a multi-stage Clinical trial in human subjects. Phase I of the clinical trials process involves taking healthy individuals and dosing them with the new drug (usually starting low and escalating). They have to look for safety, effects on the body, toxicity, side effects, maximum tolerate dose, tissue distribution, half-life and on and on. IF the drug makes it through this initial phase then it’s on to Phase II where the drug is tested in a medium size group of diseased individuals (in this case Covid-19 positive). All of this under careful supervision of doctors who are specially trained to assess dosing and efficacy. If the drug proves efficacious in this Phase II study it will move on to a larger Phase III randomized double blind study where the drug being tested is compared to a placebo control (sugar pill) to ensure that it’s really the drug having an effect. These large studies can include 1000s of people and take many years depending on the nature of the disease being tested. Finally, once a drug survives Phase III; proving safe, efficacious and with the dosing amount and regimen worked out, the company can file for approval from the FDA (1 in 5000 make it this far)(medicine.net). This whole process can take up to 12 years for chronic diseases, but of course right now things are moving much more rapidly, and a lot of the regulations and paperwork are being modified to speed up the process.
So what about all the drugs that are being tested against Covid-19 right now? There are several drugs that were identified as being potential therapeutics, and thankfully they had already passed Pre-clinical testing and Phase I trials, so this dramatically expedites the process of testing. The most promising seem to be Remdesivir (from Gilead), Favipiravir (anti-viral), and the previously mentioned hydroxychloroquine (cdc.gov, Dong et al, Wang et al). Even though all of these drugs have successfully completed varying levels of clinical trials, using them against a new disease requires a new round of efficacy, dosing and safety testing. Patients with different diseases respond to drugs differently, dosing needs to be adjusted for the new disease and of course the drug needs to be thoroughly tested to ensure that the differences seen in early studies weren’t simply because of patient selection, population bias or other factors that were not controlled for with the small sample set. In short, all these drugs, while promising, are many months away from being approved for safe use in a wide array of Covid-19 patients, if they get there at all. See the comment below from my college friend Aileen, who’s a pharmacist in the San Francisco Bay Area in response to the small test of hydroxychloroquine in patients in France (Gautret et al)….
More PSA from a pharmacist….to detail out certain claims Hydroxychloroquine used in this case is in particular HIGH DOSE (usual dose of the drug is 200-400mg daily, in this case…600mg daily and we only use that dose in Q Fever patients). When the hydroxychloroquine in high dose and azithromycin are taken together, there are risks for GI side effects…and most importantly…POTENTIAL ARRHYTHMIA. First azithromycin is a known QT prolonging agent…but also…hydroxychloroquine can either cause direct mycocardial toxicity or exacerbate underlying mycocardial dysfunction. This is a RISK that must be weighed by physicians and healthcare professionals vs. the unproven benefits. Is there promise? potentially….but we NEED MORE EVIDENCE TO EVALUATE SAFETY AND EFFICACY. Please…do not demand for it….leave it to healthcare professionals to make that decision and do our jobs….
The next question is in regards to a vaccine against Covid-19. Unfortunately, the process I outlines above for drugs, also applies to vaccines, but we’re starting from ground zero. Prior to this pandemic there were no coronavirus vaccines available (though plenty of background research), so companies have gone into serious overdrive trying to develop something, and amazingly in just two months Moderna, in collaboration with the NIH, took the first vaccine candidate to Phase I clinical trials this month (March 2020) (nih.gov). A process that usually takes 6-12 months took them 2, let that sink in for a moment. And they’re not the only company working hard on creating a vaccine, as there are numerous others with vaccine designs being tested in Pre-Clinical trials as we speak. But, this bring us back to question of time. Before a vaccine can be deployed to the general public it has many hurdles to pass, and only if it successfully passes those hurdles can it be mass produced and distributed. So, as Dr Fauci has explained many times, we’re looking at best case 12-18months for a vaccine. Guess we’re going to have to hang tight and weather this storm for a bit longer.
Seasonality
Most people have probably heard the claim at one point or another that this thing (Covid-19) is like the flu and it’ll go away when the weather warms up. Even our President claimed “…you know, a lot of people think that (the virus) goes away in April with the heat — as the heat comes in. Typically, that will go away in April.” Is there any logic or scientific evidence to support this claim? The short answer is, no, but it’s definitely more complicated than that.
The idea of seasonality was brought up because the influenza virus does see a very seasonal pattern of spread and retraction. During the cooler winter months in the Northern Hemisphere we see a dramatic rise in influenza infection rates, then a drop as the weather warms in April, as Trump suggested. There are many reasons for this; reduced contact time between people (stuck inside, schools) as weather improves, improvements in immune responses due to people being outside more and increases in Vitamin D, potential increase in duration of infection during winter months, and decreased survival of some pathogens in warmer environments (Fisman et al). While we do have the first three things going for us as they are environmental changes that aren’t pathogen specific, what about the survival time of different viruses? It’s been well documented that influenza viruses survive and transmit best at lower environmental temperatures in the range of 5C and 20C. Though starting at 20C, depending on humidity, influenza virus transmission becomes much more variable, and at 30C a dramatic decrease is seen in viral transmission (Lowen et al). Unfortunately, coronaviruses don’t seem to have the same susceptibility profile. Testing on the original SARS-CoV-1 virus showed that it was fairly stable at environmental temperatures as high as 33C (91F), and only when temperature was increase to 38C (100F) did the virus infectivity begin to dramatically drop (Chan et al 2010). SARS-CoV-2, the causative agent of Covid-19 seems to be more temperature resistant than the influenza viruses that we commonly associate with having seasonal cycles. So with the virus currently spreading in the Southern Hemisphere and in several warm weather countries we shouldn’t expect too much help with the virus from Mother Nature’s change of seasons.
But not all hope is lost! I’ve heard recently that the extreme measures taken by many states have allowed the hospitals in the US a little breathing room. Even if this is short lived it means that staff and supplies can be replenished and that buys more time for widespread testing to come on line. Countries like Germany and South Korea are good case studies for how excellent testing and surveillance can lead to minimizing the number of fatalities (testing large percentages of their populations, and doing so quickly). Even though cases and number of deaths are still increasing, we’re slowly catching up on testing, and keeping our death rate low, but the fact that we have 2,122 serious or critical Covid-19 cases is still a little scary. For now, we’re all going to have to sacrifice a bit, be more compassionate to our fellow humans and just realize that we’re living through unprecedented times, that we will get through, though it’s going to take some time. If you’re interested in reading about some potential scenarios on how the pandemic plays out in the next 3-12months this article from the Atlantic outlines them pretty well in my opinion.
Citations aytubio.com/covid-19/ cdc.gov/coronavirus/2019-ncov/hcp/therapeutic-options.html Chan et al. The Effects of Temperature and Relative Humidity on the Viability of the SARS Coronavirus. Advances in Virology, 2011. Chan et al. Serological response in patients with Severe Acute Respiratory Syndrome Coronavirus infection and Cross-Reactivity with Human Coronavirus 229E, OC43, and NL63. Clinical and Diagnostic Laboratory Immunology, 2005. Dong et al. Discovering Drugs to treat Coronavirus disease 2019 (Covid-19). Drug Discoveries and Therapeutics, 2020. Fisman et al. Seasonality of Viral Infections: mechanisms and unknown. European Society of Clinical Microbiology and Infectious Diseases, 2012. Gautret et al. Hydroxychloroquine and azithromycin as a treatment for Covid-19: results of an open-label non-randomized clinical trial. Journal of Antimicrobial Agents, 2020. Lowen et al. Roles of Humidity and Temperature in Shaping Influenza Seasonality. Journal of Virology, 2014. nih.gov/news-events/news-releases/nih-clinical-trial-investigational-vaccine-covid-19-begins unitedbiomedical.com/COVID-19/ Vincent et al. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virology Journal, 2005. Wang et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCov) in vitro. Cell Research, 2020. washingtonpost.com/world/2020/03/24/coronavirus-latest-news/ worldometers.info/coronavirus/
I’m writing this blog to detail the accident and recovery process from my dislocated elbow back in December. When I tried to find information on the recovery process and return to sports/activity, I found very little information, so hopefully this will be useful to someone in the future.
2018 ended on a little bit of a rough note as I took a fall while running down my home town trail of Gregory Canyon (on Green Mountain Boulder), smacking my elbow just right (or wrong) fully dislocating the elbow. Oh boy did that hurt like hell. I sat in the middle of the trail, taking very controlled deep breathes for what seemed like 5-10min (but could have been much longer), trying to figure out exactly what had happened. I initially thought I’d broken something, but as I probed the bones of the upper and lower arm, nothing distal hurt, and the hand, while it tingled was not numb. As we rolled up my sleeve my friend Andrea and I noticed my elbow appeared hollow, yep dislocated, and holy hell did it hurt.
One gnarly looking Xray of a text book elbow dislocation without fractures. I dislocated the elbow in flexion because of major trauma to the humerus during the fall.
Jake and Andrea used two jackets to sling my left arm to stabilize it so I could walk myself out. The final 1/2mi to the TH seemed to take forever, but with the help of a few friends I was able to slowly trudge my way out to the trailhead. For better or worse, the OSMP rangers had been alerted to my fall, so they met me at the trailhead and asked me to wait for the first responders to arrive. The firetruck pulled up, they interviewed me as I sat shivering in the cold, and once they determined I was ‘stable’ they allowed me to forgo the ambulance ride and to arrange my own ride to medical care.
Andrea was kind enough to drive me over to Urgent Care where we were hoping to get my elbow fixed, though when I described the injury the nurse said ‘nope, you need to go to the ER, because you’ll need to be sedated, given muscle relaxers, and it’s a violent procedure to relocate an elbow’….well ok then. We walked into the ER, second in line and I was soon taken back into the operating room. After some very painful X-rays (involving moving my still dislocated elbow around), I was sedated and next thing I knew I awoke, asking when they’d reset my elbow, glanced down and it was already done. They put me in a half cast, wrapped me up and sent me home with some Percocet.
I done broke myself again…argh.
Over the next week all I could do was rest the arm (in a sling) and learn to do everything else one handed. Opening pill bottles with my feet, typing with one hand, showering with a bag over my left arm, getting dressed was a fun adventure. After a week I went in for my first visit with Orthopedist, who gave me the good news that nothing was broken and nothing was completely torn (ie no surgery!). So they took the cast off and told me to move the arm around but NOT to lift anything heavier than a coffee cup. Let the rehabbing begin.
After only a week, the cast comes off, and the elbow/arm looks all kinds of nasty.
Over the next several weeks I gently used the arm for some limited activity; picking up items, typing, showering, but still very minimal weight/pressure. My range of motion had been reduced to 45-90 degrees, pretty pathetic, so I was tasked with moving the arm around and slowly working the ROM back, the most important thing to focus on in the first few weeks. After about three weeks the elbow finally began to feel stable enough so I started some easy jogging and pushing the ROM a little further. After four weeks I began some very light band work (5lb resistance), to try and reengage the atrophied bicep, tricep and forearm. By the new year I was running uninhibited, but still limited to 8lb of resistance in the left arm, so of course I did 60-100 reps of each exercise to compensate….cause that’s what you’re supposed to do right? Working not only on the bicep, tricep and forearm, but all the shoulder, back and chest muscles that had been neglected as the arm recovered. Rehab isn’t very sexy when you’ve got a 5lb weight in your hand.
Working on getting stronger however I can.
Back on the sticks finally, feels good to be out even in a limited capacity
At my 5week post-accident appointment my Dr took some additional Xrays, did some stress tests on the elbow, measured my ROM and declared me healthy enough to start weighted rehab and to increase activity. I was permitted to ski (YEAH), carefully, but to stay away from any activity that would put impact on the arm directly (volleyball and climbing) for at least another 3 weeks. So that brings me to the present day (1/16/19), where I’m now up to 12lb weights for my left arm, I’ve skied, done some wall pushups, a few assisted pullups and have increased my ROM to 10-115 degrees (a dramatic improvement). I’ve still got a lot of work to get back to full strength (still at less than 50%), but I’m getting there. The most important thing at this stage (6weeks out) is to regain the final bit of extension in my arm to straighten it, easier said than done, but with daily stretching and strengthening I’m getting there.
Weighted stretching of the elbow, trying to regain ROM 6weeks after the accident. Getting closer.
Update 1/30/19:
Now just over 8weeks out from the injury and my strength is coming back quickly. I can do assisted pull-ups without pain, push-ups on my knees (albeit with a hitch in my elbow), and even started doing some very easy bouldering. The weight and stretching actually feels good on the elbow. I’m still not at full range of motion as there is some stiffness/tightness in the joint so I’m stuck at 5degrees (not full extension) and I’m almost back to normal on the flexion side. Progress…
Update 5/14/19:
Just over 5 months after my accident I’m ‘fully’ healed, but still dealing with some lingering joint stiffness and I don’t have the last 3-5degrees of extension in my elbow, which may never come back. I’ve been back at full unhindered activity, but still rehabbing the strength and flexibility deficits. I started hitting heavier weights in late March and climbing regularly as well to help stretch the joint and strength the tricep and bicep on the left side. It’s been a slow process, but overall I no longer feel hindered, but it still feels like there’s a block in my left elbow preventing me from fully straightening the arm.
2014 started on a very somber note for the Boulder trail running community, our friend and fellow runner Marcy Servita had just been diagnosed with late stage pancreatic cancer….a diagnosis which is never good. The community rallied around her, those closest to her gave everything they could; time, energy, food, love….but on March 16th, 2014 we lost Marcy. It was a tremendous loss for the community, and obviously hit those closest to her very hard, including my friend and fellow ultra runner Greg Salvesen. Greg and Marcy had been ultra running friends (and training partners) through the Boulder Banditos running group (where we’d also met). To honor what Marcy loved (running) and as a way to cope with the loss, Greg decided to run a 100mile+ race every month in 2014…..so the story begins.
On March 16th, 2014 we lost Marcy Servitas to her battle with Pancreatic cancer.
As 2014 rolled on Greg was ticking off 100mile races as if they were 5k’s; HURT, Rocky Racoon, Antelope Island, Zion, Peak 200, Bighorn, Vermont, Fatdog…… After a hiccup with the cancellation of Mogollon Monster due to weather, Greg decided to still finish up the year’s races….though there was one issue, there were no 100mile race in December? Thanks to good friends Ryan Smith and Nick Pedatella a 100mile route was drawn up to circumnavigate Boulder, and a crew was recruited to support the run. In December 2014, supported by a crew of his friends, and joined by Ryan, Nick and a few others, they completed what became the first Boulder Badass 100 run. Since that time the Boulder Badass has become an annual event, focused on community, comradery and just doing crazy things. Fast-forward to 2018, in June I received a group message welcoming me to the 2018 version of the Boulder Badass as one of 8 participants….oh damn, I’d have only four weeks after the Grindstone 100 to recover and run yet another 100mile event.
The original Boulder Badass crew in 2014. A bunch of Dodos.
After a summer full of adventure culminating in a sub-24hour run at the Grindstone 100 (see previous post), I had four weeks to get my legs to a place where I could yet again run 100miles, by far the quickest turnaround I’d ever attempted. At 10pm on Friday Nov 2nd to the melodic reverberations of the Fart Blaster, seven of us pranced out my front door into the rainy night with only one goal…to survive the 100mile circumnavigation of Boulder before work on Monday morning. We ran head first into the cold driving rain, mud from the trails sticking to our shoes and rain threatening to soak through our jackets. Thankfully by the time we reached Dowdy Draw the rain tapered off and the stars began to break through the clouds. We fought our way around the South Boulder trails, 30-40mph winds intermittently whipping across the grasslands, just the seven of us joking around in the dark night.
A crew of dedicated friends had volunteered to crew us through the cold dark night, and were always an energetic and welcoming site for the seven of us. As we jogged our way through Walker Ranch daylight finally percolated through the cloud layer and we were able to switch off our headlamps. By the time we reached the Walker Ranch TH we were 38miles and 10hours into the Boulder Badass, but had a long way to go. The crew was ready and waiting at Walker Ranch, and we were happy to see them. We refueled, joked around then packed up and dragged our first set of pacers off onto the Meyers Gulch trail with us. We dropped down into a snow storm on Magnolia road, where Hurculean Paul ran into a dead tree at full speed knocking the 20ft tall trunk in Colleen’s direction with a huge crash, narrowly missing her. We all had a good laugh at Colleen’s near death experience, and spirits stayed high as we pounded down Magnolia road to the next crew point.
Party at the Walker Ranch Aid Station.
The gang cruising along the aquaduct toward Magnolia rd.
We arrived to quite an entourage at the base of Magnolia road, there was lots of stoke and despite having 43miles on our legs we were all moving pretty well. Next up was a little jaunt through Betasso with a whole new crew of friends hitching along for the ride. We jogged, laughed, screwed around a fair bit but kept a slow and steady pace forward. The continual stream of fresh faces joining us for Sanitas, the Hogback, Boulder Valley Ranch and finally the long haul along the bike paths back into town kept us distracted. Each time we rolled into an aid station the crowd seemed to grow, the noise decibel increased and a handful of fresh meat would join us for some miles.
The whole gang still together in Betasso. Photo by Flannery Davis.
Road side madness in Sunshine Canyon. Photo by Brendan Davis.
70miles and 20hours in we reached the Cottonwood trailhead on the East side of Boulder. I picked up Adam who was to join me for the rest of the fun filled night ahead. We had broken up into runner/pacer teams now, though none of us were far apart and I spent the boring bike trail miles leap frogging with Colleen, Paul and Doug. We all had a good laugh at the ridiculousness of our situations, the pain we were willingly enduring and as always at Doug’s endless stream of entertaining word vomit. When I rolled into Eben G Fine just after 8pm there was a serious party going on, it was a bit overwhelming for my tired brain, but I did feed off the energy a bit.
Summit of Mt Sanitas party!
Arriving at the Foothills TH to quite a welcome.
All business, or were we…..Photo by Brendan Davis
After Eben G Fine the fun began, a proper skyline traverse, with a full descent between most of the peaks to maximize elevation gain. Chapman Dr was a slog, and the mindset of most of the runners was slowly deteriorating into ultra-mush. After a little bit of confusion that had all of us taking different lines down off Flagstaff Mountain, we hit the last aid station at the Gregory TH, staggered 5-10min apart. This was our last refuel point before the long haul up and over Green, Bear and SoBo, so each of us took an extra few minutes to get our shit together. As I stood up to leave Ryan informed me that in proper Badass tradition we’d be running down Baseline Rd to Chautauqua then BACK to Amphitheater (which was currently 200ft away). In a moment of childish frustration I picked up a handful of cheese and threw it at Ryan before jogging off down the road with Adam.
Sunset from the Res, damn those peaks are far away.
I hit the climb up Amphitheater with reinvigorated legs, but just after the ladder that energy soon faded and the death march was on. Doug soon caught back up to us, greeted us with a ‘Hello Assholes’ and we commiserated our way to the summit of Green, two more summits to go. Doug and his entourage of three took off just ahead of us down Green. Fern turned out to be the slog we were all dreading. Colleen caught up to Adam and I about half way up as I drunk stumbled my way up the steep stairs, half awake, but half in a glazed over stupor. We rolled over Bear Peak and to the summit of South Boulder Peak, bypassing the crew at the saddle until the return trip. Once back at the SoBo saddle we all had only one thing on our mind, getting this shit done. I chugged a little redbull,thanked the badass volunteers who had trekked all the way up there at midnight and began the painful rock hop down shadow canyon.
“Hello Assholes”, Doug says the skyline is hard. Photo by Adam Chapman.
My feet ached with every step, the tendons in my ankles were stiff, my knees sore and my mind foggy, but with only 5miles to go it was time to get this shit done. I limped my way slowly down shadow, finally exiting the canyon only to see Jeff and Colleen’s lights coming back from the wrong direction? I made a joke to them and Colleen’s only response was something to the effect of “we went the wrong @$%* way…” and she ran off, woman was on a mission. The final few miles went by slowly, as my drive to push had faded and I was happy to power hike my way to the finish and just enjoy the cool night air. Adam and I arrived back at my house 31h54min36sec after departing on Friday night. It had been a long couple days, lots of highs and lows, lots of banter, lots of non-sense shared, and laughs had. In the end six of the seven starters had completed the entire 100mile+ course. It also turned out that the Badass was my 10th 100mile event finish, my ‘1000mile buckle’ in a sense.
Gwen overwhelmed with emotion after becoming the first finisher of the 2018 Boulder Badass. Photo Ryan Smith.
As we all lay crumpled on the floor of my living room, the only thought that came to our minds was how happy we were to be done. We were sore, exhausted, a bit delirious, but all really happy with our efforts over the past several days. The Badass had never been about beating anyone or breaking a time goal, it had been about the shared experience, the comradery and the community. While the seven of us may have been the centers of attention, the event was about bringing the local ultra community together. To support and be supported, to show that running is just running, but what makes these crazy long events so special is the community surrounding it and the friendships they foster. The Badass was created as a way to commemorate someone who left a whole in our community’s heart, but in its place was born an event that, even after five years, still emanates the love and good vibes that makes Ultrarunning so unique and amazing. This is why, even after 12years of running these things, I’m still not ready to throw in the towel, because of the support and the community that is ultrarunning.
The 2019 Boulder Badass planning has already begun. Eli is the first new participant welcomed to run.
Enjoying my 2nd 100mile burger in 4weeks. 2000 Calories of greasy goodness, thanks Southern Sun.
Finisher plaques for completing the 2018 Boulder Badass. Sweet Dodo bird fossil molds, with custom inscription. Thanks Julia & Silke!
Special thanks to all of the Rocky Mountain Runners for keeping such an awesome tradition alive and supporting us through this huge undertaking. To my fellow runners; Gwen, Colleen, Paul, Dan, Doug and Guy for sharing so many miles and all the laughs along the way. To the Godfather Greg Salvesen and the Mastermind Ryan Smith for inspiring this event (yes it’s your faults). To my pacers Nick, Josh, Derek, Mike, Aiden, Ginna and Adam…it really does take a village to raise an Idiot, and we’re especially big idiots. Lastly thanks to Vfuel for keeping me energized through this brutally exhausting two month stretch and my massage therapist Myriam Desrosiers for keeping my legs functional after all the beating they’ve taken.