
Just in case know the rules of Zombieland…
In the past several weeks the world has seen the horrible images of what the Ebolavirus can do to a human thrust into the public eye. Understandably there has been a lot of discussion, fear and misunderstanding in regards to Ebola. I’m hoping to lay out some information about the disease, assuage some fears, correct some of the misunderstanding and give the non-scientific public (or at least people I know) a glimpse into what is known about the disease.
First off, I have a Masters in Cell Biology/Immunology with a special emphasis in Infectious Disease Research. I currently do mucosal HIV research, looking at the dynamics of how HIV and the gut microbiome interact and how these interactions affect disease progression and pathogenesis. My Masters Thesis focused on the recognition of Mycobacterium tuberculosis by Dendritic Cells (a key piece of our immune system) and how the bacteria are able to corrupt our own host responses in order to avoid recognition and survive. So, in short, I have a fairly strong background in working with various infectious diseases, including Level 3 pathogens, though I am by no means an expert on Ebolavirus specifically. The thoughts below are merely my interpretations of the literature which I have read, the discussions I’ve had with others in the field, and observations on how our hospital (University of Colorado Anschutz) is preparing for this threat.
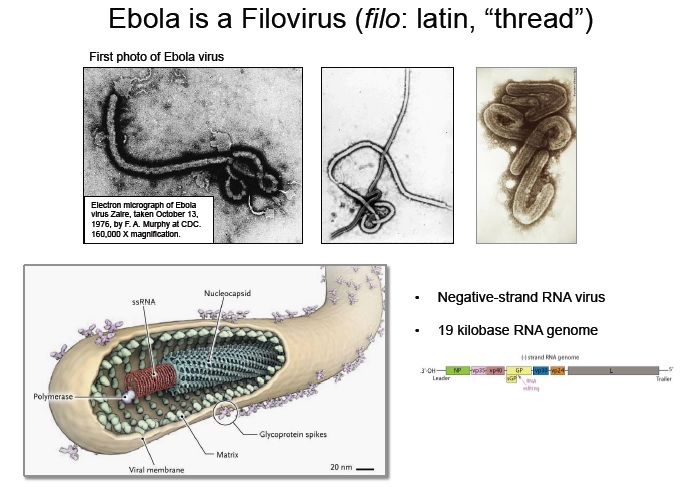
Images of Ebolavirus (top) with a schematic of its structure below.
What is Ebola?
The Ebolavirus is part of the Filoviridae family, a group of single-stranded negative sense RNA viruses. What the hell does that mean, basically it’s a virus. They are tiny structures of RNA with an envelope wrapped around the outside, they have a very basic genome, are able to form multi-virion strands (up to 6), but require the full intact structure to replicate (the RNA itself is non-infectious). There are 5 different subtypes of Ebola, each one slightly different in how virulent (infectious and deadly) it is, the current outbreak in Guinea, Sierra Leone and Liberia is caused by a variant of Zaire Ebolavirus. In most people the virus causes what’s know as hemorrhagic fever, a not so fun complex process by which the immune system is hyperactivated to such an extent that the virus literally destroys you from the inside, causing massive blood vessel leakage and organ damage. This is not a new disease, first officially discovered in 1976 in the Democratic Republic of the Congo (Zaire strain), and it has flared up numerous times in the past 40years, though the previous flare ups have all burned themselves out in more rural areas. The current outbreak has spread to the urban areas in West Africa and continues to spread uncontrolled as of this moment (10/21/14). Below I will discuss the general pathology (what happens with disease), the current state of Ebolavirus research, and what all of this means for both the US and the World (in my opinion). (Ansari AA et al 2014, Feldman H et al 2011)
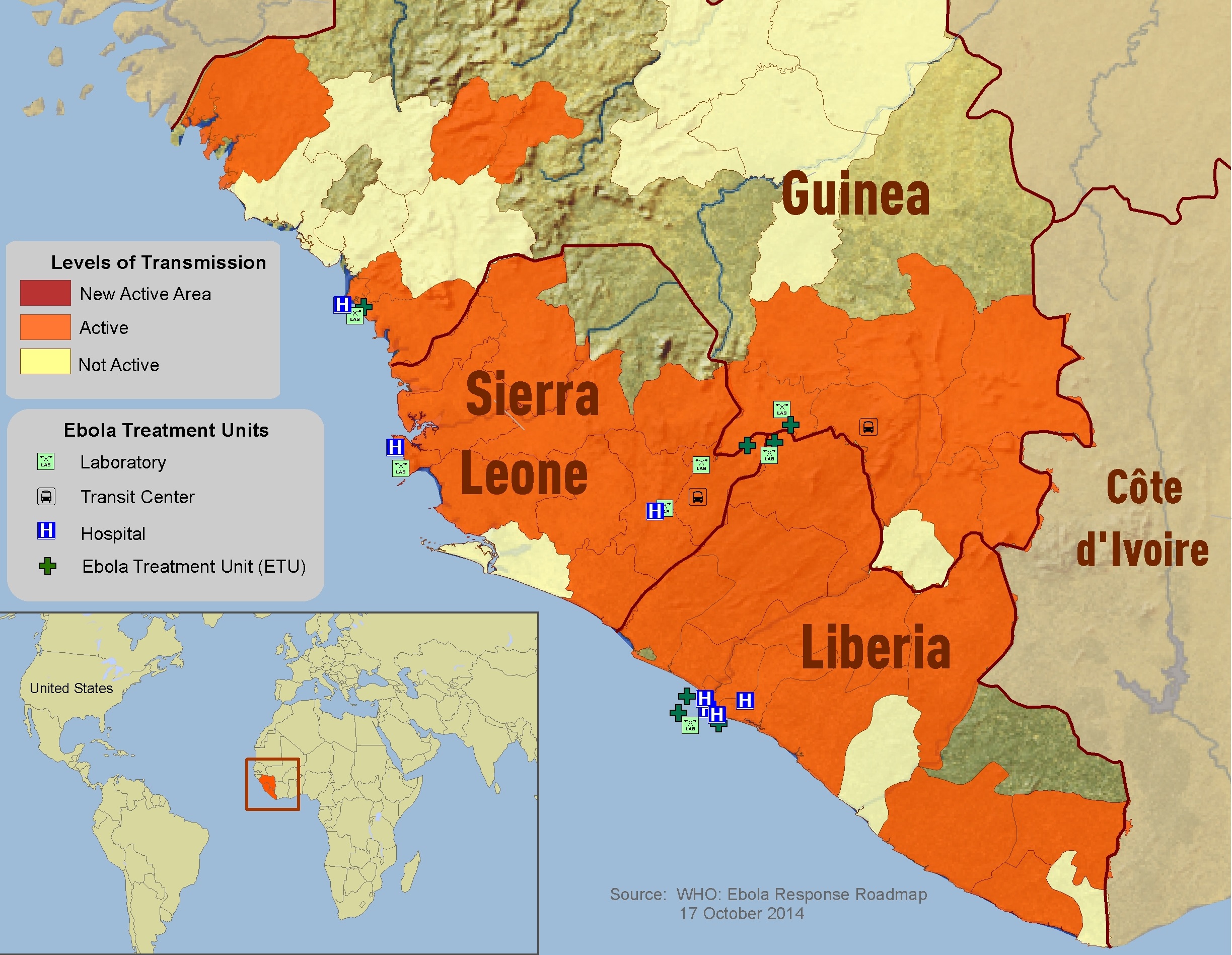
A map showing the location of the 2014 Ebolavirus outbreak. As of Oct 21st there have been over 9000 cases and 4500 confirmed deaths. Making this the largest Ebola outbreak in history.
Infection and Symptoms
The Ebolavirus, like other filoviruses, survives in and is transmitted through contact with bodily fluids such as; blood, vomit, stool, saliva, semen, urine, puss, etc. The current research and epidemiology show no evidence for generalized aersole transmission (unlike flu or cold viruses), though Ebolavirus has been shown to survive in body fluids outside of the host for several hours on surfaces, making it much easier to contract than a virus like HIV. Infection occurs when infectious materials/fluids come into contact with the mucus membranes or open wounds of a new individual (eyes, mouth, throat, nose, cuts/scrapes, etc). After infection there is what is known as an incubation period (average 4-10days), in which the virus is replicating in the individual but they don’t show any obvious signs of being sick, during this stage the new individual is not known to be infectious. During this latter part of this incubation period the initial symptoms are very general and include; fever, chills, malaise and myalgia. During the later stages of disease (typically 6-16 days) the disease takes on its more severe form in which excessive immune activation leads to coagulation disorders, blood vessel leakage, multiorgan failure and shock, often leading to death. The current Ebolavirus strain (Zaire) has a 60-90% fatality rate, though some do recover from the disease back to (apparently) full health. We still do not know exactly what leads to Ebolavirus immunity, but high levels of specific neutralizing antibodies seem to be one of the leading candidates. (Ansari AA et al 2014, Feldman H et al 2011, Hoenen T et al 2012)
Treatment Options
There are not currently any officially FDA approved vaccines or treatment options available to the general public, though there are many strong candidates in the works. Several different vaccine candidates are in development, but none have gone beyond animal trials as of this writing (Oct 2014). Several have shown very strong abilities to protect Non-Human Primates (monkeys) from infection and thus may also work in humans, TBD. Post exposure treatments are in a similar state, with several treatments having shown to be effective in animal models, but none have been extensively tested in humans. The two most common experimental treatments are the use of serum from previously immune (recovered patients) and a synthetic antibody cocktail known as ZMAPP. Both are based on the premise that specific antibodies against Ebolavirus can help the patient neutralize the infection and thus recover. All of these treatments are experimental and have NOT been extensively tested for safety and efficacy in humans, but due to the high mortality rate of Ebolavirus infection they are being used in a life saving experimental fashion. NOTE: The makers of ZMAPP are now working with Amgen to see if it would be possible to scale up its production in order to have larger quantities of this therapeutic on hand in case its needed. (Ansari AA et al 2014, Feldman H et al 2011, Hoenen T et al 2012)
Why All the Confusion?
Ebolavirus research lags behind many other disease for several reasons. One, there is not as much funding for Ebolavirus as there is for HIV, TB, and many other more prominent diseases. Two, since Ebolavirus is a Biosafety Level 4 pathogen there are only a dozen or so research laboratories that have the facilities to properly and safely study this virus. Even though the Ebolavirus research is in its infancy, it is much further along than HIV research was when the initial HIV outbreak happened in the 80s and 90s, thus there is much more promise for containing its spread.
A lot of the current fear instilled in populations of the developed world revolves around several health care workers becoming infected, and thus the concern that the virus may easily spread throughout the world. Note that just as in Africa, those becoming infected are people who have direct contact with highly infectious patients, and not simple casual bystanders. What these secondary infections in health care workers do highlight is the need for a more coordinated plan on how to deal with isolated patients in order to properly protect the care givers from the infectious virus. Many hospitals (Emory and Nebraska are two exceptions) don’t have the proper containment wards setup and Personal Protective Equipment (PPE) protocols in place to deal with an Ebolavirus infected patient if they were to walk into their facilities today. This is very disconcerting for healthcare workers who would be at high risk for transmission as they treat the patient. After the transmissions in Dallas many hospitals have implemented procedures and specific protocols on how to identify and deal with a potentially infected patient (UC Denver Anschtuz is working on this now). This is where I feel the CDC has dropped the ball the most, in not implementing an extremely detailed Nation wide protocol for hospitals on how to identify and deal with a potential Ebola case, their hospital guidelines were initially very general and in my opinion not adequate for something that is so deadly.
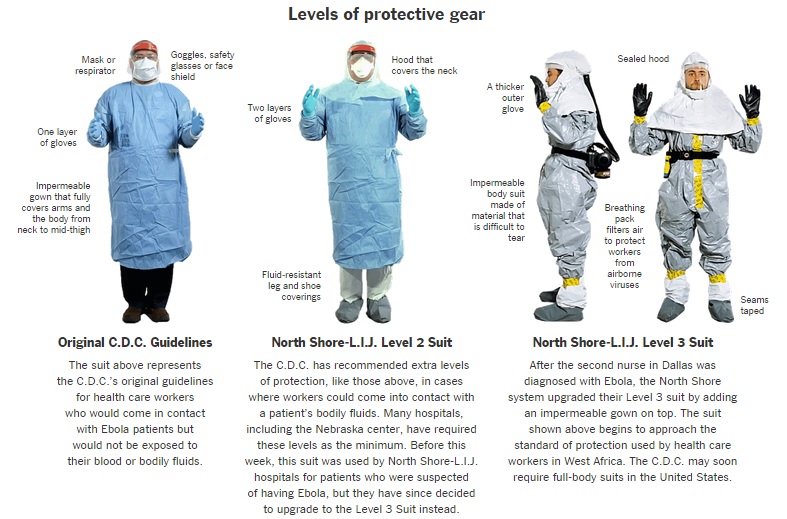
Evolution of the CDC recommended Personal Protective Equipment (PPE) for those treating Ebola patients. http://www.nytimes.com/interactive/2014/10/15/us/changes-to-ebola-protection-worn-by-us-hospital-workers.html
What Does This Mean For Me?
For most of us (me included) this outbreak in West Africa, while tragic, does not pose a direct threat to us individually. It is definitely something worth watching to see how well the CDC and WHO are able to help control the spread of the disease in the impoverished countries, but spread in the developed world has been halted by simple containment protocols and proper handling. I wouldn’t go traveling to West Africa any time soon though. If you are a healthcare worker, specifically one who works in a hospital, ER or ICU I would be more concerned until I knew my facility had the proper protocols, PPE and containment facilities in place to handle a patient potentially infected with Ebolavirus. These are the people who are at high risk because they are asked to care for the highly infectious and to put themselves directly in harms way. For now, unless you are a healthcare worker there are many more things to worry about, Ebola being quite a ways down the list. Information on the current status of the West African Outbreak, where the disease has been treated outside West Africa, and the state of the current coordinated effort on the CDCs website.
If all else fails, just remember the rules of Zombieland…
References
CDC website, http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/index.html
Ansari AA, Clinical features and pathobiology of Ebolavirus infection, Journal of Autoimmunity (2014), http://dx.doi.org/10.1016/j.jaut.2014.09.001
Feldman H et al, Ebola haemorrhagic fever, Lancet. 2011 March 5; 377(9768): 849–862.
Hoenen T, Current Ebola vaccines, Expert Opin Biol Ther. 2012 July; 12(7): 859–872.
Gatherer D, The 2014 Ebola virus disease outbreak in West Africa, Journal of General Virology (2014), 95, 1619–1624.
thanks Eric very clear and in laymans terms