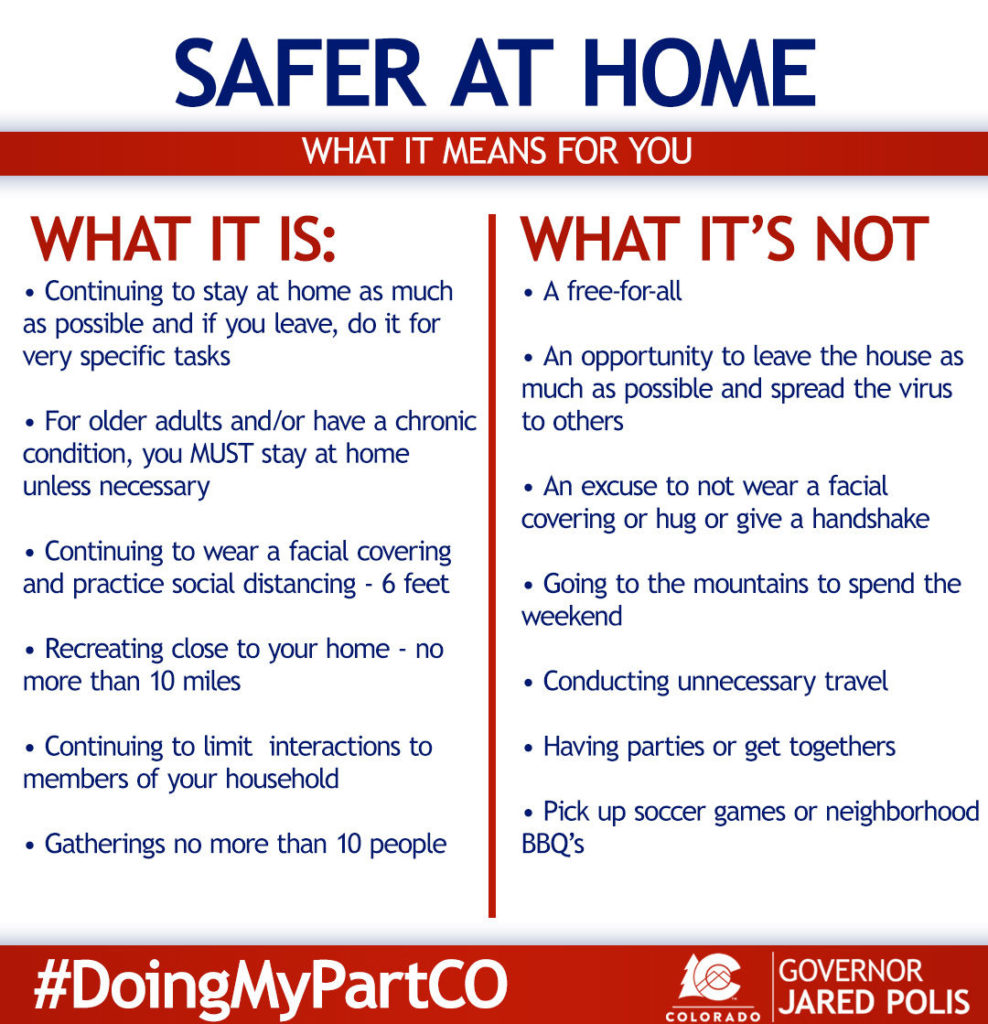
This past weekend much of the State of Colorado moved from “Stay-at-Home” to “Safer-at-Home” restrictions. This is the first step to us opening up more businesses and moving slowly back towards a state of ‘new’ normal. As part of this a lot of people across the country are preparing to go back to work (or into an office/store) in some capacity in the coming weeks. Some people think this is all BS and a hoax, you can stop reading now, for those who are worried or uncertain exactly what this return to a ‘normal workplace’ might look like, I’ll try to outline a few best practices that my work has been using and also highlight what the State of Colorado has outlined for businesses that are reopening.
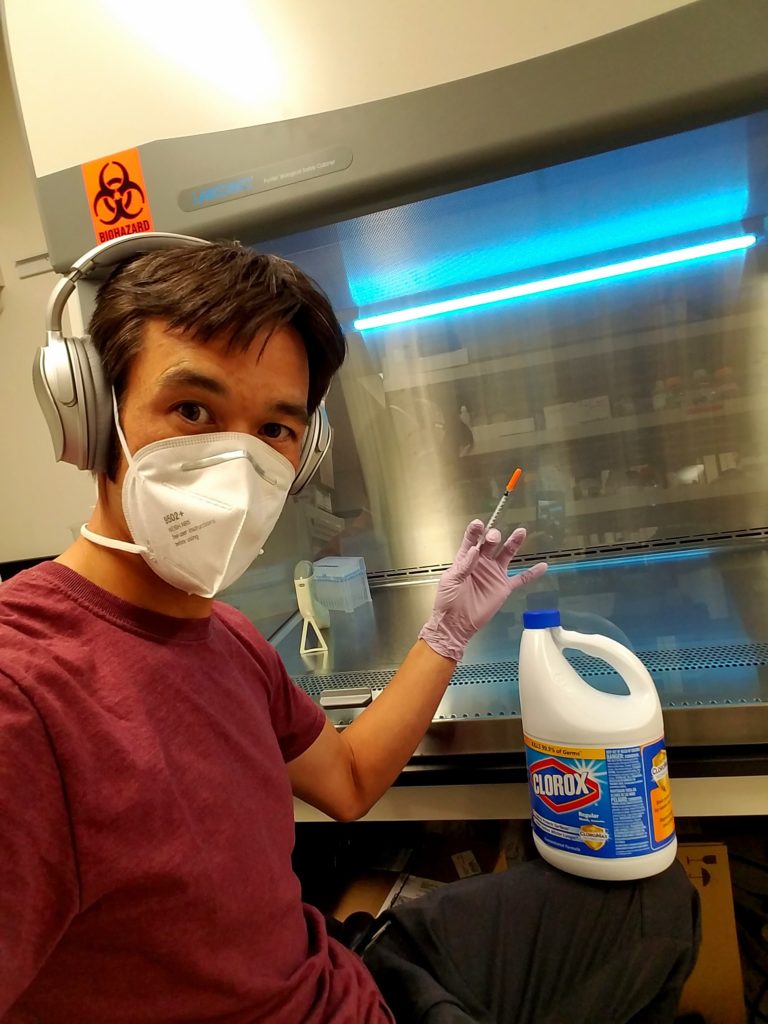
To start with for those that don’t know my background, I work in a vaccine and drug development laboratory. So my workplace will definitely look different than many of yours, but there are still many applicable practices that we’ve implemented that all types of work environments can utilize. Much of my experience in mitigating infectious hazards comes from years of working in Biosafety Level 3 facilities (with airborne, highly infectious, incurable pathogens). The stringent types of biosafety measures we implement in the lab aren’t applicable to daily life, except if you’re working in a healthcare setting in close contact with highly infectious patients (ping me separately if this is of interest to you). I’ll divide the topics up into three categories; general work place practices that should be implemented at the management level, engineering controls (equipment) and lastly how many of the common workplace practices can and should change to help you protect yourself during this uncertain time.
General Workplace Policy
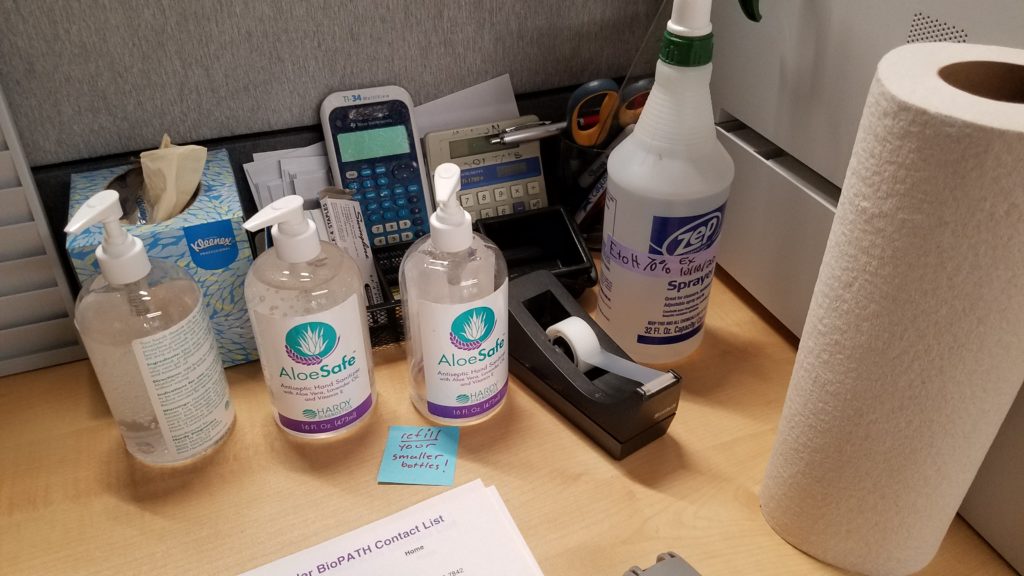
While some people can work remotely from home (best practice), many of us require specialized equipment/facilities, customer interactions or other tools that are simply not available at home. If your work place is welcoming employees back into the office/store, the State of Colorado has set out several guidelines for how work place policy should be setup to protect the employees. First, spread out the hours people work; work from home, work shifts, segregate tasks people are working on to different areas, etc. Second, the employer should be providing ample cleaning supplies, hand sanitizer and soap. In our office we also have an employee tasked with daily cleaning of the common areas and commonly touched surfaces (door knobs, time clock, fridge, conference table, etc). In addition to this I clean my personal desk each morning, it only takes a few minutes, but alleviates any concern about contamination of my immediate workspace. Third, the wearing of masks should be made mandatory for all employees (and customers) when you’re interacting with anybody else (even in passing or in the bathrooms) or moving around the office. The reason this needs to be made a company wide policy is, otherwise it’s too easy for a portion of the population to not adhere, making the effectiveness of cloth/surgical masks far less on a company wide scale, everybody needs to protect everybody else. Additionally, signage reminding everybody about the policies on staying home if you’re sick, hand washing, cleaning of common areas and wearing of masks are helpful. Many of these measures are requirements of the State of Colorado for reopening a business, check with your individual state about their requirements.
Engineering Controls
Engineering controls is a term used for physical barriers or equipment that is used to reduce the hazards of a workplace. In regards to COVID-19 in the workplace it’s referring to barriers and office setup that can help reduce interactions with coworkers and thus reduce the risk of someone getting sick. One method of limiting the workplace risk is to spread out employees desks/work spaces. Providing all employees with at least 6ft of space as to reduce the likelihood of infectious transmission. Another way is to setup barriers between employees desks/work spaces. This can be done by putting up plexiglass walls (or other materials) to block the direct line of transmission from one person to the next. So the open workspace system that so many tech companies love, is probably going to need to go away for the immediate future. Cubicles (or closed offices) actually provide a fairly safe way for each employee to have their own protected space, where infection risk is low, and you don’t have to wear a mask all the time. Work with your employer to establish these ‘safe zones’, because not only will it reduce the transmission risk, but it makes the employee far less anxious because they have their own personal space (at least in our office it works that way). For those of you working retail, store fronts or other customer based jobs, many of these rules won’t directly apply. My recommendation would be to establish a safe zone for yourself (back room, office, car, outside). Take breaks to get out of the mask for a few minutes (pretend like you’re a smoker) or just to step into the back room/warehouse for a few minutes to relax and breath. Plan and prepare for the long haul.

Common Workplace Practices
While the previous two sections mostly addressed changes that can/should be broadly implemented in the workplace, this section is going to address how the actions of individuals/groups should change. I have a feeling for many people this is going to be the hardest section to incorporate into our daily lives, but these changes are equally as important as those above. The first one is simply an extension of the general social distancing policy that pervades our lives, but applied to the workplace. No group lunches, standing around the coffee/espresso machine, office parties, etc (yes, sad face, I know). It doesn’t mean you can’t chat with coworkers or socialize, but it does mean it has to be done at a safe distance apart and while wearing your masks. If/when you need to use common office equipment (printers, coffee makers, fridge, cash register, etc) either make sure the equipment is well cleaned off or sanitizer/wash your hands afterwards as a precaution. This mitigation measure may be slightly less important for some workplaces, and more important for others (depending on how many people you’re sharing space with). On the far end of the spectrum are people whose jobs require direct contact with others (massage therapist, physical therapist, hair stylist, acupuncturist). For these professions it’s even more important to sanitize all surfaces after each client, wear masks (tough for hair salons), make sure both client and provider clean their hands before interacting, and of course pre-screen your clients to make sure they are not sick or symptomatic.
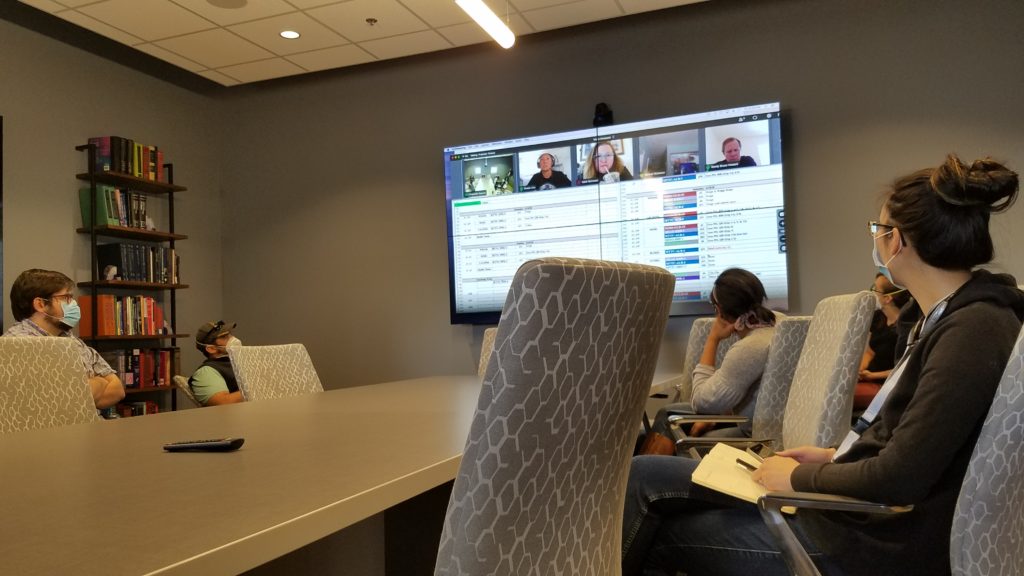
The last one is probably fairly obvious for many people, but meetings are going to look quite a bit different (if they happen at all). The easiest way to mitigate the risk is to do virtual meetings (Zoom, Skype, Teams, etc) whenever possible. Of course sometimes it’s much faster and more efficient to meet in person, which can definitely be done very safely. The smaller the better to start with, but as meetings grow, ensure there is at least one seat between everybody in the room, and everybody continues to wear their masks when in the same room.
Final Thoughts
My office/lab implemented most of these procedures the first week of Colorado’s Stay at Home order and shutdown. We have our own cubicles/workspaces that are our own private areas when we’re not working in the common lab spaces. We wear gloves (because it’s a lab) and masks whenever working in close proximity to others, common surfaces are regularly cleaned, our employees with COVID-19 risk factors spend much of their time working from home, or working off shifts, our meetings are done half virtual half in person (with masks). Using all these measures we’ve had no issues with viral transmission and also minimal issues slowing down our workflow. If you or your employer are hesitant to implement many of these actions, just look at the extreme cases of the meat packing plants all over the country. They stayed open but didn’t implement any infection risk mitigation (employees working in close quarters), and ended up suffering large outbreaks forcing their businesses to shutdown. So it’s really in everybody’s best interest to protect themselves and those around them, to stay healthy and keep the business running without the major setbacks that an outbreak would cause.
While company wide policy is up to the employer, you are your own strongest advocate. So it’s important to assess your work place (and how it operates) and how best to mitigate risks. If an employer isn’t providing you at least the minimum levels of protection outlined above, then speak with your local public health department, as they will come in and further assess what more can and should be done. Going back to work in and of itself isn’t a problem, it’s doing so in a responsible and controlled manner that allows your workplace to implement and test out these new policies. For all businesses there will be a trial period of adjustment to the new way of functioning, just be flexible and understand most of these changes really don’t dramatically affect our lives (and definitely don’t impinge our our civil liberties), we’re all going to get through this.
State of Colorado general Guidelines
State of Colorado Guidelines for Protecting Workers and Customers
Definition of Lab Biosafety Levels
CDC Guidelines for Businesses (far less specific than individual states)